Mindfulness Meditation Improves Health
In one study conducted at the Wake Forest Baptist Medical Centre in North Carolina, scientists found that doing meditation daily for a few minutes could relieve pain better than a powerful pain relieving medication.
What is meditation? If you've followed my blog here (or if you browse earlier posts) you know that my approach to meditation is quite simple and straightforward. Although I have studied theology and philosophy seriously, including the great religions, I do not see meditation through the lens of religion. Like contemplative prayer, however, meditation has the capacity to soothe, calm, and relax the mind, and the most challenging aspect of meditation is simply to practice on a daily basis.
Meditation is the simple practice of making the mind calm, and silent, and bringing your thoughts to one point. In other words, meditation can be defined as making mind free from agitation, turning attention away from distracting thoughts and focusing on the present moment. Some individuals incorporate meditation as part of religious practice, and others do not. Yoga, for example, is one approach to meditation that has spiritual roots, and the same is true of contemplative prayer in Christian and Jewish traditions. Zen meditation, deriving from Buddhism, also has spiritual aspects.
Christian writer Phil Fox Rose says, "The promise of a devoted spiritual life, of which meditation is an invaluable part, is serenity...that in everyday life you will not be anxious, restless or irritable; and that in good times you will be fully alive to enjoy them."
After practicing meditation for even a few weeks, what many people notice is that mindfulness becomes a part of everyday life. In other words, we become more mindful in every activity. We focus more clearly, we think and speak more in terms of the present moment, and we act with greater compassion and clarity.
Meditation produces many benefits. I have noticed that my meditation practice improves concentration, strengthens the mind and leads to multiple health benefits: lowering blood pressure, reducing emotional distress , diminishing anxiety attacks, and improving my relationships.
The Wake Forest study now shows that meditation each day could be better in relieving pain than taking morphine. Similar studies at Duke and Harvard point to similar findings.
In their study, the lead researcher, Dr. Fadel, examined the brain scans of individuals who had been trained to use relaxation and breathing techniques to cope with the pain. After studying the brain scans, his team noticed that the study subjects who meditated regularly had calmer brain scans. They saw a 27 percent reduction in pain intensity and 44 percent less emotional pain in group of volunteers who actually practiced mindfulness meditation.
Along with many others, I believe that such findings prove that mindfulness meditation can produce different patterns of brain activity to suppress the feeling of pain.
Based on the study results, the scientists believe 20-minute a day meditation practice could be added to conventional pain relief methods for better and quicker relief. The study focused on volunteers who were pain free, so the question remains as to whether individuals with more serious pain problems can achieve similar results. The study findings are reported in the Journal of Neuroscience.
Another study from the Department of Psychiatry at Duke University Medical Center shows that mindfulness meditation can protect against depression. There are now hundreds of scientific papers on mindfulness. A Harvard Medical School study showed promising results in pain relief: "Recently, it has been demonstrated that pain can also be attenuated by mindfulness….Mindfulness practitioners and controls received unpleasant electric stimuli in the functional magnetic resonance imaging scanner during a mindfulness and a control condition. Mindfulness practitioners, but not controls, were able to reduce pain unpleasantness by 22% and anticipatory anxiety by 29% during a mindful state."
Let me know if you discover new findings in this exciting area of research!
What Are Marijuana "Dabs"?
A dab usually refers to a dose of concentrate that is heated on a hot surface, usually a nail, and then inhaled through a "dab rig." It doesn't sound so controversial in those terms, but “blasting dabs” has become a dividing point within the community both because of the intense high that it produces and for the image that it presents to outsiders.

A Dab Rig Sold Online
What are Dabs and How are They Made?
Dabs are concentrated doses of cannabis that are made by extracting THC and other cannabinoids using a solvent like butane or carbon dioxide, resulting in sticky oils also commonly referred to as wax, shatter, budder, and butane hash oil (BHO). While it's possible to extract non-psychoactive compounds like CBD, THC is what's behind the potent effects of dabs, making them the fastest and most efficient way to get really, really medicated. Terpenes, or the aromatic oils that give cannabis flavor, can also be extracted, although it can be difficult to preserve these volatile compounds in the extraction process.


From http://leafly.com
What are the Concerns Surrounding Dabbing?
Here's what the Leafly website says about dabbing: "Let’s start with the bad news first: dabbing can be dangerous. Actually, it’s the extraction that can be dangerous.The process can be tricky, but thanks to online forums and videos, many amateur "scientists" think they have mastered the technique enough to try it on their own. In cases when things go well, the product is probably still pretty poor. When things go bad, houses blow up. When I worked out in rural Texas, people were getting blown up when cooking methamphetamine in their kitchens. Today, there are other ways (like extracting cannabis oil) that apparently can get you blown up as well.
"Another side effect of these home extraction experiments is “dirty” oil that may contain chemical contaminants that could present health hazards to consumers. If the concern is butane, the dangers are most likely minimal since it already occurs in everyday products such as scent and flavor extracts. Whether or not the equipment used in the extraction process is adding additional contaminants is a more viable issue. When done correctly, these extras can be avoided, so as is the case with growing cannabis, it’s best to leave it to those who know what they’re doing.
"One of the most unsettling facts about dabs is that thanks to the super-concentrated power of BHO, for the first time it seems possible to “overdose” on cannabis. While still not lethal, taking more than your personal limit of dabs can lead to uncomfortable highs and, in some cases, passing out. After all of the chanting that “you can’t overdose on marijuana,” concentrates could be undermining advocates’ message of safety. There have also been reports of more intense withdrawal symptoms for dabbers, but again, the information is limited."
For more on recent research on potential problems with marijuana, see my previous post (scroll down here on the blog) "Update on Marijuana Research."

Pain Pill Addiction: Basics
Breaking free of prescription drug abuse takes much more than willpower. As I often say, "You have to do it yourself, but you can't do it alone." There are individuals who claim to have "kicked" or achieved abstinence without any help, but I don't know many of them. Early on, before dependency sets in, it's possible to recognize the problem and stop using narcotics. Once dependence sets in, though, it's not so easy.
Fortunately, medications and counseling can improve the chances of success. Newer drugs like buprenorphine (sometimes combined with naloxone) and naltrexone and traditional therapies like methadone and 12-step programs, are helping thousands of people stay on the road to recovery.
Physical Dependence and Detoxification
Narcotic addiction leads to real changes in certain areas of the brain. Prescription drug addiction alters the circuits responsible for mood and "reward" behaviors.
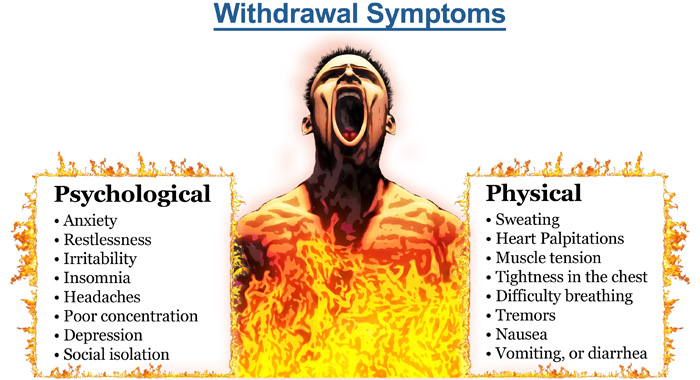
In addition, long-term prescription drug abuse affects virtually all the systems in the body. Cutting off the supply abruptly leads to opioid withdrawal symptoms.
Symptoms of opioid withdrawal include:
- Craving for drugs
- Diarrhea
- Large pupils
- Yawning
- Abdominal pain
- Chills and goose bumps (the origin of the phrase "cold turkey")
- Nausea and vomiting
- Body aches
- Agitation and severe negative moods
A list of symptoms doesn't capture the agony of opioid withdrawal.
The syndrome is intensely unpleasant, and people will do almost anything to avoid it.
Opioid withdrawal lasts from hours to several days -- and sometimes weeks -- depending on how long and how much a person has used their drug of choice. After the intense initial symptoms subside, some physical and mental discomfort may persist for weeks.
Medications for Opioid Withdrawal
Opioid withdrawal is difficult to endure, and is a major reason for relapse and continued prescription drug abuse. Medications are used to prevent symptoms of opioid withdrawal during detox, easing the person out of physical dependence:
Methadone is a long-acting opioid drug. It activates the same opioid receptors as narcotics, effectively eliminating withdrawal symptoms. Providing the correct dose of methadone prevents opioid withdrawal symptoms and eases drug craving but it does not provide the euphoria. The dose can be slowly tapered off, freeing the person from physical dependence without withdrawal symptoms. Methadone is the most effective known treatment for narcotic addiction.
Buprenorphine and Naloxone (Suboxone) is a newer combination drug that helps for detox from prescription opioid addiction. Buprenorphine activates opioid receptors, reducing drug craving and preventing withdrawal. Naloxone helps prevent misuse of the medication.
Clonidine is a blood pressure medicine that acts on the brain. Clonidine reduces the effects of the "fight or flight" response, which is over-activated during opioid withdrawal. However, clonidine does nothing to reduce drug craving, and is mostly ineffective when used alone.
"Rapid detox" programs claim to accelerate the process of detox and opioid withdrawal by giving large doses of opioid blocking drugs. Some programs place an addict under general anesthesia during the detox process. These programs have not proven to be more effective than traditional methods of detox, and may be more dangerous.
Maintenance Therapy After Detox
Completing detox subdues the physical effects of narcotic addiction and opioid withdrawal. But experts say psychological and social factors are the main drivers that push addicts back to using. Stress and situations that remind the brain of the drug's pleasure are common triggers.
When drug cravings strike, they can be impossible to resist. Most people who go through detox and short-term counseling will relapse to prescription drug abuse.
Studies show that the chances of beating narcotic addiction are better with long-term maintenance therapy with either methadone or buprenorphine paired with naloxone (Zubsolv, Bunavail, Suboxone) . These drugs are used during the maintenance phase of treatment. People on these drugs are still opioid-dependent, but they are often freed from their destructive drug addiction. They can return to work, drive without impairment, and function normally in society. Naloxone has also been combined with oxycontin ( Targiniq ER ) to deter abuse by snorting or injecting the drug. A person can still become addicted by taking it orally, however.
Methadone is the best-studied, most effective method of recovery from narcotic addiction. Suboxone, while newer, has gained wide acceptance as maintenance therapy.
Some people have a high rate of relapse when maintenance therapy is stopped, and so they remain on the medicines for decades. In others, maintenance therapy is tapered off over months to years.
Naltrexone (ReVia, Vivitrol) is an opiate receptor-blocking medication used in maintenance therapy for narcotic addiction. Unlike methadone and Suboxone, naltrexone does not activate receptors at all, so it does not reduce opioid withdrawal or craving. However, because naltrexone blocks opiate receptors, a person won't get high if he or she uses drugs while taking the medicine. The drug is usually ineffective by itself, because people can simply stop taking it and get high shortly after.
Counseling and 12-Step Programs
Narcotics Anonymous (NA) is an international network of community-based meetings for those recovering from drug addiction. Modeled after Alcoholics Anonymous (AA), NA is a 12-step program with a defined process for overcoming narcotic addiction.
NA is an abstinence-based program. In principle, NA is opposed to the use of maintenance therapy. Methadone Anonymous is a 12-step program that acknowledges the value of methadone or Suboxone in recovery from narcotic addiction. Methadone Anonymous has caught on in California, but I don't know much about meetings in Texas. If you have information about Methadone Anonymous meetings, contact me.
Most of us who are experts in the field recommend participation in a 12-step program or other form of counseling. Therapy can take place as an outpatient, or in a residential facility. I discuss the value of 12 Step Programs on my FAQ page.
Update on Marijuana Research
According to a recent analysis presented at the 2015 Meeting of the American Chemical Society, the amount of THC in samples from marijuana sold in Colorado are reaching 30 percent. Three major patterns have emerged over the past few months since Andy LaFrate, Ph.D., and his lab began testing marijuana samples. Those patterns concern potency, amounts of a substance called CBD and contaminants in the products.
“As far as potency goes, it’s been surprising how strong a lot of the marijuana is,” LaFrate says. “We’ve seen potency values close to 30 percent THC, which is huge.” LaFrate is the president and director of research of Charas Scientific, one of eight labs certified by Colorado to do potency testing.
THC is an abbreviation for tetrahydrocannabinol, which is the psychoactive compound in the plant. He explains that three decades ago, THC levels were well below 10 percent. Its content has tripled in some strains because producers have been cross-breeding them over the years to meet user demands for higher potency, he says.
But an unexpected consequence of this breeding has occurred, says LaFrate. Many of the samples his lab has tested have little to no cannabidiol, or CBD. CBD is a lesser known compound in marijuana that is of increasing interest to medical marijuana proponents. Researchers are investigating CBD as a treatment for schizophrenia, Huntington’s disease and Alzheimer’s disease. It is also being considered for anxiety and depression. But unlike THC, CBD doesn’t get people high — that’s a key trait for many people who are wary of buzz-inducing drugs and for potential medical treatments for children. As for recreational users, the lack of CBD in marijuana means that many of the hundreds of strains they select from could in actuality be very similar chemically, according to LaFrate.
"What we have today is not the weed we used to smoke in the 1960's."
In a recent report researchers found that the concentration of THC sold on the streets in Denmark has tripled to an average of 28 percent in the last 20 years.
Attitudes toward marijuana are also rapidly changing. In the 1960s surveys found a mere 12 percent supported marijuana legalization—now, more than 50 percent are in favor. Over the past decade recreational/medicinal use of cannabis was legalized in the District of Columbia as well as in Alaska, Colorado, Oregon and Washington State; 19 other states also permit the use of the drug for medical purposes. As more states and countries, such as Canada and the U.K., consider following suit, advocates and critics are engaging in heated debates about the potential risks and rewards—particularly in light of the increasing prevalence of highly potent marijuana. But the evidence is nebulous—even within the scientific community, there is lack of consensus about how much harm marijuana can do to users’ brains and mental health.
In addition to THC, the other major component of marijuana that has caught the attention of researchers is cannabidiol (CBD), which scientists have linked to antipsychotic properties. Not only do THC and CBD have opposing effects, cannabis with higher THC content tends to contain lower amounts of CBD. “The relationship between CBD and THC is unique, in that the biological process required to make THC antagonizes the generation of CBD,” says Matthew Hill, a cannabinoid neuropharmacologist at the University of Calgary.
Damage to the brain?
In an article published last month in Psychological Medicine, researchers conducted a neuroimaging study to assess the effects of cannabis use on the corpus callosum, the largest collection of white matter in the brain containing fibers that facilitate communication between the two hemispheres. They found that this structure was negatively affected in those who used high potency cannabis—strains high in THC and low in CBD—compared with those who used lower strength bud or did not use at all. Moreover, the changes were similar in both those with and without previous episodes of psychosis. However, the researchers assert that they did take other drug usage into account.
Previous studies have demonstrated the importance of these confounding factors when interpreting marijuana’s effects on the brain. For example, a 2014 study in The Journal of Neuroscience reported that marijuana use was associated with changes in brain structures associated with reward processing. This effect was dose-dependent, meaning the more cannabis someone used, the more changes became apparent in their brains. In a subsequent study, published in 2015 in the same journal, another group of researchers found that once variables such as alcohol use, gender and age were controlled for, the differences between users and nonusers disappeared.
Marijuana madness?
In a study published earlier this year in Lancet Psychiatry the same group of researchers at King’s College found that using cannabis, and THC specifically, can produce acute psychotic symptoms, and some researchers suggest it increases the risk of developing schizophrenia. The link between marijuana and psychosis, however, has been a matter of heated debate in the scientific community. Researchers have argued that there are sufficient grounds to doubt the causality of this link. There are two alternative possibilities: being predisposed to schizophrenia may increase the likelihood for cannabis use or a third variable may make it more likely for people to use marijuana and develop schizophrenia. For example, previous studies have suggested that schizophrenia and cannabis share both genetic and demographic risk factors, such as low socioeconomic status.
Critics also point to the fact that all the studies to date have been correlational. But this does not immediately dismiss the possibility that causation is possible. After all, although there was a strong correlational link between smoking and cancer, it took a study of more than 30,000 British doctors to confirm causality.
According to Haney, the odds ratio—the likelihood that an exposure will lead to a certain outcome—of marijuana causing psychosis are much lower than those for smoking and cancer. “There is also an association with tobacco smoking and schizophrenia that is much stronger [than cannabis use],” Haney says. “If this relationship is causal, it is a tiny effect, which might explain why there hasn't been a dramatic upsweep in rates of schizophrenia in recent years.”
Both Haney and Evins agree that it is biologically plausible that marijuana, particularly at a young age, could increase the likelihood of negative psychiatric outcomes. The developing brain has an abundance of cannabinoid type 1 (CB1) receptors, where THC binds to exert its effects, in the prefrontal cortex, a key brain area impacted by schizophrenia. “I don't think it's a good idea for young children to be smoking marijuana at all because of their developing brains but I am extremely cautious about pinning it all on marijuana when there is a potential for many other explanations,” Haney says.
To truly determine whether marijuana causes such effects, scientists would need to track changes that occur in a large number of individuals before and after they use a drug over a long period of time. An effort to conduct this type of study is currently underway—the National Institutes of Health recently funded the multicenter Adolescent Brain Cognitive Development Study, which plans to recruit 10,000 children before they start drug use, and follow them for 10 years to assess the short-and long-term effects of using marijuana, tobacco and other drugs.
Teenagers and young adults at risk?
Cannabis has been found to impair cognitive functions such as memory and is increasingly being considered an addictive substance, especially in adolescents. There are still many questions that remain to be answered but strict regulation and lack of funding pose large barriers to conducting the required studies. The U.S. Drug Enforcement Administration still classifies marijuana in its most restrictive “Schedule I” category, which puts tight regulations on researchers who want to study its effects.
A New Zealand study found that persistent cannabis users show neuropsychological decline from childhood to midlife. These scientists found that frequent and persistent marijuana use starting in adolescence was associated with a loss of an average of 8 IQ points measured in mid-adulthood. Significantly, in that study, those who used marijuana heavily as teenagers and quit using as adults did not recover the lost IQ points.
Users who only began using marijuana heavily in adulthood did not lose IQ points. These results suggest that marijuana has its strongest long-term impact on young users whose brains are still busy building new connections and maturing in other ways. The endocannabinoid system is known to play an important role in the proper formation of synapses (the connections between neurons) during early brain development, and a similar role has been proposed for the refinement of neural connections during adolescence. If confirmed by future research, this may be one avenue by which marijuana use during adolescence produces its long-term effects. (For details see: Meier MH, Caspi A, Ambler A, et al. Persistent cannabis users show neuropsychological decline from childhood to midlife. Proc Natl Acad Sci USA. 2012;109:E2657-2664.)
The ability to draw definitive conclusions about marijuana’s long-term impact on the human brain from past studies is often limited by the fact that study participants use multiple substances, and there is often limited data about the participants’ health or mental functioning prior to the study. Over the next decade, the National Institutes of Health is planning to fund a major longitudinal study that will track a large sample of young Americans from late childhood (before first use of drugs) to early adulthood. The study will use neuroimaging and other advanced tools to clarify precisely how and to what extent marijuana and other substances, alone and in combination, affect adolescent brain development.
Scientists agree the highly potent marijuana may be better to avoid. Aside from potential long-term harm, receiving a high dose of THC can be especially risky for first-time users who are more likely to experience adverse effects such as panic or anxiety attacks. But even knowing the potency of a product, consumers might not always get what they ask for.
Because of competing laws at the state and federal level, the quality of regulation varies largely between states and regions. Although THC potency labeling is mostly required for both medical and recreational products, it is not always accurate—a study published this June in JAMA The Journal of the American Medical Association revealed that of the 75 edible marijuana products (from 47 different brands) researchers assessed only 17 percent accurately labeled their THC content.
The article states: "Edible cannabis products from 3 major metropolitan areas, though unregulated, failed to meet basic label accuracy standards for pharmaceuticals. Greater than 50% of products evaluated had significantly less cannabinoid content than labeled, with some products containing negligible amounts of THC. Such products may not produce the desired medical benefit.
"Other products contained significantly more THC than labeled, placing patients at risk of experiencing adverse effects.5,6 Because medical cannabis is recommended for specific health conditions, regulation and quality assurance are needed.
"A limited number of cities, dispensaries, and products were included. Because no source lists all dispensaries, and many products are not labeled with cannabinoid content, a true random sample was not possible and the results may not be generalizable. However, this study illustrates the variability in label accuracy for edible cannabis products within 2 of the largest medical cannabis markets in the United States."
Across labs and in homes, marijuana remains a highly debated issue. Marijuana is an extremely polarizing topic among scientists, as these articles demonstrate. My own view is that marijuana is not likely to cause someone to suffer a schizophrenic illness, but clearly what we have today is not the weed we smoked in the 1960's.
Random Facts on Happiness
I've collected various facts about happiness. Here are a few of them, with a little help from my friends at WebMD:
Californians are not terribly happy. Out of 51 slots, California ranks No. 46 on the happiness scale. Surprisingly, New York and California do badly in the happiness ranking. Researcher Andrew Oswald of the University of Warwick in Coventry, England, says, "Many people think these states would be marvelous places to live, but the problem is that if too many individuals think that way, they move into those states, and the resulting congestion and house prices make it a non-fulfilling prophecy." So where is the No. 1 place brimming with happiness, you ask? Louisiana!
It's a fact: People are happier, less stressed, and feel better about themselves after age 50! A recent survey of more than 340,000 people showed overall feelings of well-being improve as people pass middle age. Negative emotions such as stress and anger decline after the early 20s, and people over 50 worry less than younger folks. Researchers say it may be as simple as this: With age comes increased wisdom and emotional intelligence.
In terms of happiness, a boost in your mood is linked to the release of serotonin, endorphins -- your body’s "feel good" chemicals -- and oxytocin, also known as the "love/comfort/compassion" hormone. Tryptophan helps your body make serotonin, so it’s linked to feeling good, too.
Good news for folks whose bedrooms have more activity than their bank accounts: Research shows that sex is better for your happiness than money. Overall, the happiest folks are those getting the most sex: married people, who report 30% more between-the-sheet action than single folks.
Dopamine is a feel-good chemical that’s involved in pleasure. A study found that when people listened to music, their brains released more dopamine. In fact, even just thinking about listening to music caused the dopamine to start flowing. The researchers think this might explain why music -- from Beethoven’s Fifth to Adele’s "Rolling in the Deep" -- has been such a big part of human history.
Having a positive outlook doesn't mean you never allow yourself to feel sad. "Happiness is not the absence of sadness," says David Spiegel, MD, medical director of the Center for Integrative Medicine at Stanford University School of Medicine. It is not a stiff upper lip or the pop psychology mantra, intoning "always stay upbeat" no matter what. "Phony happiness is not good." By suppressing sadness, you suppress other, more positive emotions, as well, he says. So people who try to suppress emotions actually become more anxious and depressed.
Sure, pleasure is great and you need plenty of it, though there is more to happiness than racking up pleasurable experiences. Psychologists studying the effects of positive emotions say gratitude can boost our sense of happiness if we turn it into a conscious and regular practice. Feeling gratitude, they say, is something you do (such as expressing gratitude or keeping a gratitude journal), not something you wait for!
Some studies have found that laughter may boost infection-fighting antibodies and immune cells in the body. And when scientists at the University of Maryland studied the effects on blood vessels when people were shown either comedies or dramas, they found that the people who watched dramas tended to tense up, restricting blood flow. The people who watched comedies had normal blood flow.
Recognizing Bullshit!
Our lecture was designed to show that psychiatry, like many other professions, engages in "a great deal of bullshitting when it comes to human nature and personal experience." Needless to say, the talk stirred a bit of controversy, and the medical school was not quite sure how to advertise the event.
The concept of "bullshit," however, is quite relevant in psychiatry and philosophy, as Professor Harry Frankfurt has pointed out in his essay, "On Bullshit," which is included in his wonderful book of essays, The Importance of What We Care About. That book, as much as any other, has influenced my life and work for many years. I refer to it in a brief paper published in the Journal of Philosophy, Psychiatry, and Psychology.
Dr. David Scales has written a terrific article published on WBUR's CommonHealth, and I really got a kick out of this, so I offer it here in full. In the online article, the editors had to take out the word "bullshit" and replace it with BS, so I have taken the liberty of using the actual word, for obvious reasons.
Deep? Or Pseudo-Profound Bullshit? Psychologists Explore Why Some Can’t Tell
What do you think of the following sentences?
“The universe is the wisdom of objective external reality.”
“Experiential truth embraces the expansion of actions.”
“Death is only possible in intrinsic possibilities.”
Are they profound wisdom? Or are they bullshit? If you thought they were profound, you might need your bullshit detector checked.
Created from the website wisdomofchopra.com, this “wisdom” was generated by randomly putting together words found in the tweets of Deepak Chopra, the physician and author.
Who is more likely to see such bullshit as profound? And why? These are the questions that motivated Gordon Pennycook, a psychology PhD student at the University of Waterloo in Ontario, Canada, and his colleagues to publish a paper this week called “On the reception and detection of pseudo-profound bullshit.” (They spelled out the full word, which academic psychology allows but the AP Stylebook we use does not.)
The researchers took quotes like those above and tested whether people could see pseudo-profound statements for what they were — bullshit. Their findings suggest that people with higher intelligence and better critical-thinking skills are likeliest to detect bullshit. And more than one-quarter of the population they studied were particularly prone to buying in to it — and to holding, shall we say, “alternative” beliefs on topics from medicine to magic.
At first, this may seem like -- you know -- bullshit, but Gordon Pennycook is a real person. [Yes, Pennycook is his real name, despite its similarity to “poppycock.”] And if you wonder whether studying susceptibility to bullshit is important, just consider the possible effects on everything from votes in next year’s election to purchases of purported cure-all supplements.
The paper, published in the journal Judgment and Decision Making, is a remarkable study, not only in profane language — using the word bullshit about 200 times — but also in finally applying empirical analysis to the study of bullshit. Much has been written about it previously, but mostly just musings on the topic: “bullshit about bullshit,” Pennycook joked.
Bullshit hasn’t always gone by that name. It has been variously called crap (Hemingway), humbug, mumbo-jumbo, hot air, gobbledygook, hogwash, claptrap, woo-woo, baloney (Carl Sagan), bunk, poppycock or Orwellian doublespeak. “The fact that we have so many words for bullshit shows how pervasive it is,” Pennycook said.
What is it exactly? First defined by Dr. Harry Frankfurt, author of the best-selling book “On Bullshit,” it is different from lying, in which people deliberately manipulate or subvert the truth. Instead, bullshit statements are designed to sound impressive but have no regard for the truth.
As the authors of the study note, “it attempts to impress rather than to inform; to be engaging rather than instructive.” Think politics, advertising or bureaucratese. As Carl Sagan put it, “credulous acceptance of baloney can cost you money…but it can be much more dangerous than that, and when governments and societies lose the capacity for critical thinking, the results can be catastrophic.”
What Makes Us Susceptible?
We all think that we have highly attuned bullshit detectors, probably from years of listening to politicians. But the key questions that psychologists are trying to understand are: What makes some people more prone to seeing bullshit as profound? Are there personality traits, like open-mindedness or Sagan’s critical thinking, that incline someone toward being more accepting or skeptical of it?
In various experiments, the researchers asked participants to rank various short phrases from 1 to 5, giving higher numbers to more profound statements. Some statements were manufactured bullshit, like the tweets above. Some were mundane, like “Most people enjoy some sort of music.” And some were profound, like “Your teacher can open the door, but you must enter by yourself.”
“We speak of bullshit artists and spin doctors. To call it
artistry implies originality, innovation and creativity.”
– Philosopher Harry Frankfurt
Most participants could detect bullshit statements, and could easily differentiate mundane phrases from truly profound phrases. But some had difficulty weeding out the pseudo-profound from actually profound motivational statements. A full 27 percent gave bullshit statements a score of 3 or more.
What made them more prone to believing the bullshit was profound? To test that, the researchers followed the initial experiments by doing cognitive testing on the participants to assess their intelligence, and asked about spiritual leanings, views on conspiracy theories and alternative medicine.
They found that people who were less analytic and had lower cognitive ability were more prone to confuse the bullshit for the profound. That wasn’t all; those people were “more likely to hold religious and paranormal beliefs, and are more likely to endorse complementary and alternative medicine.”
In short, it looks like Carl Sagan’s intuition was right. Critical thinking may be your best defense against bullshit.
The Father Of Bullshit Studies
Why is it worth developing ways to study bullshit empirically in the lab? It’s the next step in a field that has taken off thanks to a seminal text that turned out to be a watershed: Dr. Frankfurt’s “On Bullshit“. Originally published in an obscure journal article in 1986, underground buzz led Princeton University Press to publish it as a small book in 2005. It reached No. 1 on The New York Times Bestseller List, spending 27 weeks there. Today, the book has been cited over 600 times.
“It was a concept I was using quite freely but I didn’t really know what it meant,” Dr. Frankfurt, now an emeritus professor of philosophy at Princeton University, said in a phone interview. “As an analytical philosopher, it’s my job to clarify and illuminate concepts like that.”
We need to study bullshit because we seem to have a higher tolerance for it than for lying, he argues. “We may seek to distance ourselves from bullshit, but we are more likely to turn away from it with an impatient or irritated shrug than with the sense of violation or outrage that lies often inspire,” he noted in his original article. For some reason, it doesn’t seem to violate our expectations of polite society.
Perhaps our tolerance is already explained by how we talk about it. “We speak of bullshit artists and spin doctors,” Dr. Frankfurt told me. “To call it artistry implies originality, innovation and creativity.”
The book’s unlikely success could probably be chalked up to both the ubiquity of the concept in our daily lives and its profanity. The word itself carries power. “It was very provocative to see a book by an Ivy League professor dealing with such a topic,” he told me. “I made the topic respectable in a way.”
That power to provoke also struck Pennycook. “There is force behind the word "bullshit" that implies, ‘We’re not OK with this,’ ” he said. “I think we should be forceful with our labels.”
The study authors specifically looked at “pseudo-profound bullshit.” That may sound redundant, but, as the authors note, it is only one type of bullshit. Thinking quickly, you can easily come up with other examples of bullshit. For me, the card game characterized by bluffing and “bullshitting your way through” comes to mind, and particular situations (like college, an interview or life itself.) Others have written about various types: pomposity or fanaticism, pseudoscientific nonsense or academic writing which has no regard for meaning.
To test the pseudo-profound sort, the researchers needed to be able to create bullshit— at will. It turns out, that’s the easy part. Profound-sounding but ultimately meaningless sentences are everywhere on the Internet. There’s the Twitter hashtag #cosmicconsciousness or wisdomofchopra.com. They also included quotes from the New Age Bullshit Generator, which is a load of fun.
(I hope you weren’t planning on getting anything else done today besides wasting time on fake pseudo-profound, new age tweets. You’re welcome.)
To explain how a psychology paper about bullshit ends up on a health blog: It is worth noting that the two bullshit generators for this paper were both inspired by quotations from Chopra, who is a physician. I’ve never read any of his books, so I cannot say whether his writings are bullshit, but profound-sounding misinformation is unfortunately all too common in health and medicine. Think about the late-night infomercials selling diet pills or vitamins. The wary health consumer should always be on the lookout for bullshit.
An interesting footnote: “On Bullshit” was translated into at least 16 languages. Dr. Frankfurt recalled that for some of them, like French, Russian, Portuguese and Hebrew, no exact equivalent for the term “bullshit” could be found, so they used the term “bullshit” spelled out in their own alphabet.
“I don’t understand how languages can get along without it,” he said. “It’s not as if the phenomenon is unknown to them.”
Learn About Your Brain!
Are you curious about what goes on inside your head? Every thought and action is controlled by the brain — the body’s most complex organ. The brain is divided into functional units with particular tasks, like processing visual information or responding to fearful experiences. Each of these units is made up of brain cells that work together. These cells also form connections with cells in other functional units, creating communication routes for brain signals.
Using new tools to tag and trace brain circuits, scientists are working to better understand how the human brain is organized to perform its many functions. Ongoing studies in animals and people are helping scientists recognize the many different types of brain cells and the roles they play. In addition, imaging technology is helping map brain regions responsible for specific functions and behaviors.
A great introduction to the different parts of the brain is on the Brainfacts website here. A much more detailed source for images of the brain can be seen here.
BROKEN BRAINS ADVANCE NEUROSCIENCE
In this podcast from Science Friday, science writer Sam Kean joins Ira Flatow to talk about the brain injuries that led to some of neuroscience’s biggest breakthroughs. From “H.M.,” who lost his memory during surgery, to Phineas Gage, whose grisly encounter with a tamping iron put him into high school psychology books, Kean explains how the field of neuroscience emerged from stories of brains gone awry.
AND WHAT ABOUT ADDICTIONS?
Addiction is a chronic brain disease that causes people to lose their ability to resist a craving, despite negative physical, personal, or social consequences. People seek out nicotine and alcohol, or engage in gambling, because it makes them feel good or lessens feelings of stress and sadness. Many abused drugs produce a pleasurable feeling by exciting cells in the brain’s reward center.
With repeated use, drugs can change the structure of the brain and its chemical makeup. But why can some people casually drink alcohol or smoke cigarettes, while others fight to kick the habit?
Neuroscience research, both in human and animal studies, is helping scientists identify key factors that influence susceptibility to addiction, such as a person’s genetic makeup, vulnerability to stress, and the age they start engaging in the behavior. Slowly but surely, new studies are unraveling clues about processes in the brain that influence the likelihood of drug relapse. Such insights may help improve rehabilitation programs and drive down the global cost of addiction.
Watch the video about brain chemistry and addiction here.