Stages of Change: A Summary
Stages of Change
The Stages of Change, as described in the treatment of alcoholism and other addictions, can be summarized in five parts. The stages are best conceptualized as a cycle. Alcoholics and addicts cycle through the stages, sometimes three or four times, before they complete the cycle without a slip or a relapse. This can be very frustrating for all concerned. But that's the nature of the game.
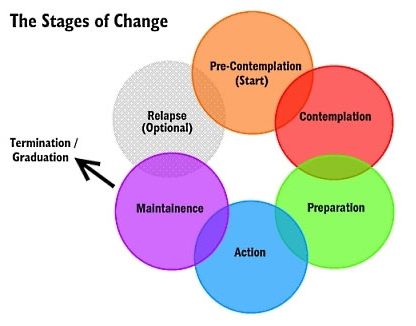
1) PRECONTEMPLATION STAGE
"It isn't that we can't see the solution. It's that we can't even see the problem for what it is."
Pre-contemplators usually show up in therapy because of pressures from others: spouses, employers, parents, and courts. They resist change. When their problem comes up, they change the topic of conversation. They place responsibility for their problems on factors such as genetic makeup, addition, family, society, destiny, the police. They explain how little they actually use or drink, and they complain that no one gives them credit when they cut down or even abstain for a short time. They feel hopeless and demoralized, and they are often defensive, angry, and frankly illogical in their thinking.
2) CONTEMPLATION STAGE
"I want to stop feeling so stuck. I am tired of all the hassles and of other people intruding in my life."
Contemplators admit that they have a problem and begin to think about solutions. Contemplators struggle to understand their problems, to see its causes, and wonder about possible solutions. Many contemplators have indefinite plans to take action within the next few months. They know where they want to do, and they have ideas (some good, some not so good) about how to get there.
"You know your destination, and maybe even how to get there, but you're not ready to go…yet."
Contemplators tell themselves that someday they are going to change. When contemplators are trying to reach the preparation stage of change, their thinking is clearly marked by two changes.
First, they begin to think more about the future than the past.
The end of contemplation stage is a time of anticipation and anxiety. Relapse is common when individuals reach this stage. They are fearful of what will happen next. Support from family and friends may be exhausted. Even though they have made considerable effort, things often don't get easier — not yet.
Between stage 2 and 3: A decision is made. People conclude that the negatives of their behavior outweigh the positives. They choose to change their behavior. They make a commitment to change. This decision represents an event, not a process.
3) PREPARATION STAGE
Most people in the preparation stage are planning to take action and are making the final adjustments before they begin to change their behavior. Usually they have not resolved their ambivalence. A part of them wants to get well, but as the Zen saying puts it, "The mind is a barrel of wild monkeys," and they often go back and forth about taking action.
4) ACTION STAGE
The time for action does not come on with a blinding flash of light. There is no burning bush. Gradually the person overtly modifies his or her behavior and his or her surroundings. At this point the make the move for which they have been preparing. This is a critical point, and it requires the greatest commitment of time and energy.
Change is visible to others. Others can see the difference in attitude, honesty and commitment. Small changes sometimes matter the most.
5) MAINTENANCE STAGE
Change never ends with a single action. One old saying in Alcoholics Anonymous is that without a strong commitment to maintenance, there will surely be relapse, usually to the pre-contemplation or contemplation stage.
THE IMPORTANCE OF PROCESSES
Processes are selected activities that are regularly initiated to effect change. There are nine important ones chosen by therapists as distinct areas of consideration and useful tools in personal transformation.
1. Consciousness-raising: Increasing knowledge about yourself and your problem.
2. Social liberation: Considerations in the external environment that can contribute to helping change, i.e.: no smoking areas, lo-cal menu items, advocacy groups.
3. Emotional arousal: Increased awareness through depth of feeling from natural events or dramatic intervention, psychodrama.
4, Self-reevaluation: A thoughtful and emotional reappraisal of yourself as regards your problem, weighing the pros and cons of changing.
5. Commitment: Acknowledging that you are the only one who can respond, speak and act for yourself.
6. Countering: Planning for and substituting healthy responses for unhealthy ones, action oriented.
7. Environmental control: Restructuring your personal environment so that the probability of a problem-causing event is reduced.
8. Rewards: Affirmation of desirable behavior by self or others as contrasted with and better than any type of punishment for problem behavior.
9. Helping relationships: Receiving care, support and assistance from significant people in your life.
For more information about the stages of change, see the book Changing for Good by James Prochaska.
Mindfulness Therapy: Alternative to Antidepressants
Mindfulness-based cognitive therapy aims to change the way people think and feel about their experiences. How we think affects how we feel. And the use of mindfulness practice is relatively easy for most people. Just 10-15 minutes two or three times daily makes a difference. The current study compares MBCT with maintenance antidepressant medication for reducing the risk of relapse in depression. The results are encouraging.
The study aimed to establish whether MBCT is superior to maintenance antidepressant treatment in terms of preventing relapse of depression. Although the findings show that MBCT isn't always more effective than maintenance antidepressant treatment in preventing relapse of depression, the results, combined with those of previous trials, suggest that MCBT may offer similar protection against relapse or recurrence for people who have experienced multiple episodes of depression, with no significant difference in cost.
"Mindfulness gives me a set of skills which I use to keep well in the long term. Rather than relying on the continuing use of antidepressants mindfulness puts me in charge, allowing me to take control of my own future, to spot when I am at risk and to make the changes I need to stay well." — Study Participant
MBCT builds on the insight that when people with a history of depression experience even a brief period of feeling low they tend to be especially vulnerable to negative thinking. That negative thinking is often accompanied by what’s known as “processing biases”: worrying about past problems, for example, or returning to unpleasant memories. Thinking like this raises the risk of a full-blown depressive episode.
MBCT focuses on helping people to become more aware of these thoughts and feelings, and thus better able to gain distance from them. As its founders put it: “We discover that difficult and unwanted thoughts and feelings can be held in awareness, and seen from an altogether different perspective – a perspective that brings with it a sense of warmth and compassion to the suffering we are experiencing.”
Talk Therapy? Medication?
I am an old-timer, and when my generation trained in psychiatry virtually all of us planned on being psychotherapists who were well educated in the use of medication as an adjunct to talk therapy. All psychiatrists I knew back then had been in psychotherapy themselves; personal therapy was considered part of becoming a competent clinician: "Physician, know thyself."
If a psychiatrist has a limited vocabulary, and can't conjugate nouns and verbs, how can they possibly communicate with patients?
Research shows that when psychotherapy and medication are both available, the combination is synergistic. It's like saying 1 + 1 = 3. Today, however, fewer than 10% of psychiatrists are trained and skilled in psychotherapy. My opinion is that this is why a good psychiatrist is very hard to find. I have been teaching young psychiatrists for over thirty years, and I have been a training director in one of our finest medical schools, and I can say with authority that many psychiatrists coming out today get failing grades when it comes to important skills like writing, speaking, and communicating clearly. I'm talking about basic errors in English grammar, syntax, and sentence structure — the stuff most people should learn by the time they enter high school! If a psychiatrist has a limited vocabulary, and can't conjugate nouns and verbs, how can they possibly communicate with patients? This is one reason that psychiatrists today are, in general, poor psychotherapists with little interest in what talk therapy has to offer.
Writing in a medical chart is similar to text messaging. It's easy, and grammar doesn't count. In fact, the modern electronic medical record discourages thoughtful writing, just like text messaging does. A good psychiatrist should not only speak well and write well. A good psychiatrist should be a superior thinker and communicator. Every doctor should have a big sign on the wall behind the chair where the patient is sitting: "DOCTOR, YOUR PATIENT IS TRYING TO TELL YOU SOMETHING!"
Here's Dr. Friedman again: "With few exceptions, every major class of current psychotropic drugs — antidepressants, antipsychotics, anti-anxiety medications — basically targets the same receptors and neurotransmitters in the brain as did their precursors, which were developed in the 1950s and 1960s."
"Sure, the newer drugs are generally safer and more tolerable than the older ones, but they are no more effective."
Prescribing a pill is easier and cheaper than offering the patient psychotherapy. Psychiatrists are paid more to prescribe pills than to counsel with patients. It is understandable, then, that the incentive is to see five patients in a single clinic hour. This saves insurance companies a lot of money. Many insurance companies will not even pay for psychotherapy with a qualified psychiatrist. And think about this: if a patient doesn't like the psychiatrist, there are fewer repeat or return visits. The winners are the insurance companies.
Dr. Friedman is also critical of trends in research, not because they are wrong, but because of simplistic logic. "The doubling down on basic neuroscience research" he says, "seems to reflect the premise that if we can unravel the function of the brain, we will have a definitive understanding of the mind and the causes of major psychiatric disorders." He points to an editorial in May in one of the most respected journals in our field, JAMA Psychiatry, emphasizing the brain but not mentioning the mind, the complexity of mental illness, or anything about how psychotherapy scientifically helps the brain. Friedman believes that "an undertaking as ambitious as unraveling the function of the brain would most likely take many years. Moreover, a complete understanding of neurobiology is unlikely to elucidate the complex interactions between genes and the environment that lie at the heart of many mental disorders."
"Anyone who thinks otherwise should remember the Decade of the Brain, which ended 15 years ago without yielding a significant clue about the underlying causes of psychiatric illnesses."
—Professor and Psychiatrist Richard Friedman
Dr. Friedman's article generated a number of replies, including this one from Christopher Lukas, a noted author:
"Over the years, I have had talking therapy for my depression and post-traumatic stress disorder, and I don’t believe I would be alive were it not for those sessions. I have also taken a whole range of medications for depression and find that psychotherapy outweighs the benefits of any of those drugs.
"Some psychiatrists and some patients think that drugs are better because they work like aspirin: Take two and call me in the morning. But, as Dr. Friedman pointed out, and as I have experienced, other patients find doses of talking therapy can work well if we’re patient and if we understand that many emotional problems may take time to go away.
"Persistence, willingness to give yourself over to the process and willingness to change therapists if the talk isn’t helping you: These are key to talk therapy’s benefits."
The comments by Lukas remind me of something I pointed out to a patient just last weekend. Asking about Alcoholics Anonymous, she wanted to know what it takes to succeed in finding sobriety through AA. "An easy way to think about it," I said, is to remember the three letters H-O-W." The old AA acronym stands for "honesty, open-mindedness, and willingness."
Another writer, who is a physician herself, also agreed with Dr. Friedman:
"For the past 30 years psychotherapy has been given short shrift as drug therapy has become the treatment of choice. There are many reasons for this, but the most powerful are economic.
"Doctors can manage medication for many more patients in a day than they can treat with psychotherapy. More important, pharmaceutical companies, which profit from the drug sales, support research, thus providing funds to psychiatry departments that receive no similar support for psychotherapy research. Sadly, in the past generation or two there has been a huge loss in professional expertise as fewer psychiatry residency programs provide top-notch psychotherapy education and supervision.
"Twenty-eight years ago I went to medical school planning a career in child psychiatry. My interest had been primed by fascinating conversations I’d heard in high school between my father, a psychoanalyst, and his colleagues. My medical school psychiatry rotation was a disappointment. There was no attempt to solve the riddles of patients’ emotions and behavior, only the adjustment of medication doses to treat symptoms. Still wanting to solve puzzles, I chose a career in radiology.
"When my father died, I was tremendously moved to hear some of his patients who attended his funeral tell me how the treatment he provided had profoundly changed their lives. Psychotherapy should be an integral part of psychiatric training."
Since I do both — I am a psychotherapist who prescribes medication when appropriate — it's understandable that I agree with Dr. Friedman. It's also true that I practice this way because that approach provides the best care for the brain, the mind, and the whole person.
Best Therapists = Best Outcomes (by far)
Those Danged Cognitive Distortions
1. ALL-OR-NOTHING THINKING: You see things in black-and-white categories. If performance falls short of perfect, you see yourself or others as total failures.
2. OVERGENERALIZATION: You see a single negative event as a never-ending pattern of defeat. Phrases like "You always …" or "You never …" exemplify overgeneralization.
3. MENTAL FILTER: You pick out a single negative detail and obsess on it so that your vision of all reality becomes darkened, like the drop of ink that discolors an entire glass of water.
4. DISQUALIFYING THE POSITIVE: You reject positive experiences by insisting they "don't count" for some reason or other. In this way you can maintain a negative belief that is contradicted by your everyday experiences. Often this manifests as making excuses when somebody pays you a compliment.
5. JUMPING TO CONCLUSIONS: You make a negative interpretation even though there are no definite facts that convincingly support your conclusion often a "wait and see" attitude is called for in these situations.
• MIND READING: You arbitrarily conclude (usually by personalizing their behavior) that someone is reacting negatively to you, and you don't bother to check this out.
• THE FORTUNE TELLER ERROR: You often anticipate that things will turn out badly, and you feel convinced that your prediction is an already-established fact.
6. MAGNIFICATION (CATASTROPHIZING) OR MINIMIZATION: You exaggerate the importance of things (such as your achievements or someone else's goof up), or you inappropriately shrink things until they appear tiny (your own character defects or other people's acceptable behavior). This is also called the "binocular trick."
7. EMOTIONAL REASONING: You allow your negative emotions to color how you see the world with an "I feel it, therefore it must be true."
8. SHOULD STATEMENTS: You try to motivate yourself or others with should and shouldn't, as if needing be whipped and punished before you could be expected anything. "Musts" and "oughts" are also offenders. The emotional consequences are guilt. When you
direct should statements toward others, you feel anger, frustration, and resentment as do they!
9. LABELING AND MISLABELING: This is an extreme form of overgeneralization. Instead of describing your error, you attach a negative label to yourself. "I'm a loser." When someone else's behavior rubs you the wrong way, you attach a negative label to him "He's a dumb jerk!" Mislabeling involves describing an event with language that is highly colored and
emotionally loaded, and generally not factually descriptive.
10. PERSONALIZATION: You see yourself as the cause of some negative external event, which in fact you were not primarily responsible for.
My generation of psychiatrists was the first to break with the old-fashioned, unscientific model known as Freudian psychoanalysis—the stereotype of the patient lying on the couch for years and being "analyzed" by the shrink. For some reason, our generation just didn't see this as very helpful or useful. Psychoanalysis in its pure form means 4-5 visits a week to the psychoanalyst, and the typical course of therapy is measured in years! There were no outcome studies proving the effectiveness of this approach. We really wanted something that would produce results, and an approach that the average person could afford.
Dr. Ben Martin at PsychCentral describes the new, scientific talk therapy this way: Cognitive behavioral therapy (also known by its abbreviation, CBT) is a short-term, goal-oriented psychotherapy treatment that takes a hands-on, practical approach to problem-solving. Its goal is to change patterns of thinking or behavior that are behind people’s difficulties, and so change the way they feel. It is used to help treat a wide range of issues in a person’s life, from sleeping difficulties or relationship problems, to drug and alcohol abuse or anxiety and depression. CBT works by changing people’s attitudes and their behavior by focusing on the thoughts, images, beliefs and attitudes that we hold (our cognitive processes) and how this relates to the way we behave, as a way of dealing with emotional problems.
An important advantage of cognitive behavioral therapy is that it tends to be short, taking four to seven months for most emotional problems. Clients attend one session per week, each session lasting approximately 50 minutes. During this time, the client and therapist are working together to understand what the problems are and to develop a new strategy for tackling them. CBT introduces them to a set of principles that they can apply whenever they need to, and which will stand them in good stead throughout their lives.
Cognitive behavioral therapy can be thought of as a combination of psychotherapy and behavioral therapy. Psychotherapy emphasizes the importance of the personal meaning we place on things and how thinking patterns begin in childhood. Behavioral therapy pays close attention to the relationship between our problems, our behavior and our thoughts.
Being Mindful and Positive
Mindfulness is natural, but we often overlook the importance of living in the present moment. There is not much new to learn; it's more about being aware of what is happening, who we are, and how to practice. We already have the capacity to be present, and it doesn’t require us to change who we are. You will hear me describe, in our conversations, topics like attention, awareness, empathy, compassion, being in the zone, situational awareness, presence, flow, contemplation, and many more. Being mindful has the power to change how we approach ourselves, our work, our relationships, and our communities. Mindfulness practice should be part of everyone's toolbox in the process of recovery from any mental or emotional setback. On my links page I have listed some useful resources on the subject.
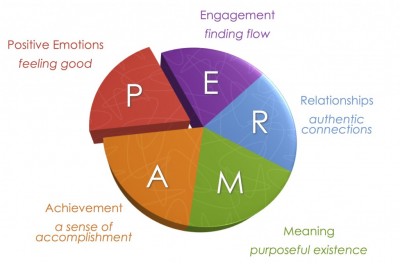
Positive psychology began to emerge in the late 1980's through the research of my colleague Dr. Martin Seligman. If you have attended my talks on the positive psychology of addiction recovery, you've heard me describe "PERMA," the five dimensions of life where positive psychology produces meaningful results. Seligman outlines the categories in his book, Authentic Happiness. The acronym for the five elements of Seligman’s well-being theory is PERMA (Positive Emotions, Engagement, Relationships, Meaning and purpose, and Accomplishments).
What people in addiction recovery notice, usually right away, is the strong similarity between the findings of positive psychology research and the guiding principles of twelve step recovery.
Positive emotions include a wide range of feelings, not just happiness and joy. Included are emotions like excitement, satisfaction, pride and awe, amongst others. These emotions are frequently seen as connected to positive outcomes, such as longer life and healthier social relationships.
Engagement refers to involvement in activities that draws and builds upon one’s interests. Mihaly Csikszentmihalyi explains true engagement as flow, a feeling of intensity that leads to a sense of ecstasy and clarity. The task being done needs to call upon higher skill and be a bit difficult and challenging yet still possible. Engagement involves passion for and concentration on the task at hand and is assessed subjectively as to whether the person engaged was completely absorbed, losing self-consciousness.
Relationships are all important in fueling positive emotions, whether they are work-related, familial, romantic, or platonic. We receive, share, and spread positivity to others through relationships. They are important in not only in bad times, but good times as well. In fact, relationships can be strengthened by reacting to one another positively. It is typical that most positive things take place in the presence of other people.
Meaning is also known as purpose, and prompts the question of “Why?” Discovering and figuring out a clear “why” puts everything into context from work to relationships to other parts of life. Finding meaning is learning that there is something greater than you. Despite potential challenges, working with meaning drives people to continue striving for a desirable goal. The three criteria are that it 1) contributes to well-being, 2) is pursued for its own sake, and 3) is measured independently of the other elements of PERMA.
Accomplishments are the pursuit of success and mastery. Unlike the other parts of PERMA, they are sometimes pursued even when it does not result in positive emotions, meaning, or relationships. Accomplishment can activate the other elements of PERMA, such as pride under positive emotion.Accomplishments can be individual or community based, fun or work based.
The five domains are valuable to consider when "the program isn't working," because taking personal inventory usually comes down to looking at what's going on inside these categories. The five elements were sifted out of research on thousands of individuals who were interviewed on the broad topic of happiness.
Changing the Brain
People with chronic fatigue syndrome (CFS) tend to have a decrease in a type of brain tissue called grey matter in the prefrontal cortex of the brain. OCD researchers in the Netherlands provided 16 sessions of CBT, and found significant increases in gray matter volume in the prefrontal cortex. This seems to suggest that the CFS patients were able to “recover” some gray matter volume after CBT.
The bottom line: Although medication and psychotherapy appear to work their magic in difference places, the results are positive for both. The mechanism of action remains unclear, but studies also show that the combination of psychotherapy and the right medication (getting it right is very important!) is an excellent approach for many individuals. As the brain changes, we see the production of new proteins, which change our brains through neuroplasticity. In selecting a treatment strategy, sometimes medication works best, sometimes psychotherapy is the best option, and sometimes it’s a combination of the two.
Identifying the Effective Psychiatrist
Practicing medicine is a privilege granted to very few individuals, and I am indeed fortunate. Within the field of medicine, working in psychiatry requires more than an understanding of anatomy and organ systems, because psychiatry is about the mind, the brain, the self, and human experience.
Like any other professional, I believe in high ethical standards, sound knowledge of my field, and the importance of practicing wisely and compassionately. Beyond the obvious nostrums and philosophical cliches, however, I want to be one of the good psychiatrists. As I thought about this lately, I began to wonder: how does one identify and recognize a really good psychiatrist? What makes a good psychiatrist? If I made a list of the most important aspects of a psychiatrist’s professional philosophy, what would that look like?
In 2006 an article was published in the Journal of Affective Disorders showing that good psychiatrists prescribing placebos (sugar pills) had better results than poor psychiatrists prescribing actual medication. Over 120 patients were divided into two groups, one group that received sugar pills and another group that received full strength psychiatric medication for depression. At the same time, each psychiatrist was rated on a number personal qualities: verbal fluency, interpersonal perception, expressiveness, warmth, acceptance, empathy, and the ability to focus on the other person. When results were analyzed, the psychiatrists strong in these personal qualities had the best results, even when the “medication” they prescribed was not medication at all.
The effective psychiatrists were fluent, clear, and expressive in speaking, and they had an accurate feel for their patients. Rather than being distant and aloof, the good psychiatrists were warm, friendly, and accepting. The good psychiatrists empathized well, spent more time with their patients, were more thoughtful in their strategies, and formed strong therapeutic partnerships. The point of the study was that having a good psychiatrist makes a difference in recovery.
Although medication can be extremely helpful in psychiatric care, treatment is not all about medication. The combination of the right medication, the right psychotherapy, and the right psychiatrist is the key to success.
Research has shown for generations that some clinicians consistently produce better results than others, regardless of the type of psychotherapy or theoretical orientation of the practitioner. Hundreds of studies have shown that the differences between types of psychotherapy is very small, but the psychiatrist providing the psychotherapy is critically important.
Over the past fifteen years, extensive research has given us a solid body of evidence about the qualities and actions of effective psychiatrists. Based on the psychotherapy research of Dr. Bruce Wampold of The University of Wisconsin, I have formulated here an inventory that provides the basis for judging whether a psychiatrist is likely to be effective.
- Effective psychiatrists demonstrate a sophisticated set of interpersonal skills, including verbal fluency, perceptiveness of others, emotional intelligence, expressiveness, warmth, and acceptance. Given these gifts, the most effective psychiatrists are those who are first excellent physicians, well trained in medicine, competent to practice at the highest levels.
- Effective psychiatrists are inquisitive, questioning, and seeking new knowledge constantly. They embrace science while at the same time possessing the humility to know how little we really know.
- Patients of effective psychiatrists feel understood, trust the psychiatrist, and believe the psychiatrist can help. The psychiatrist creates these conditions in the first moments in both speech and action. In the initial contacts, patients are very sensitive to cues of acceptance, understanding, and expertise. Although these conditions are necessary throughout therapy, they are most critical in the initial interaction to ensure engagement in the therapeutic process.
- Effective psychiatrists are able to form a working alliance with a broad range of patients. The working alliance involves the therapeutic bond, but also importantly agreement about the task of goals of therapy. The working alliance is described as collaborative, purposeful work on the part of the patient and the psychiatrist. The effective psychiatrist builds on the patient’s initial trust and belief to form this alliance and the alliance becomes solidly established early in therapy.
- Effective psychiatrists provide an acceptable and practical explanation for the patient’s distress. The patient wants an explanation for his or her symptoms or problems. There are several considerations involved in providing the explanation. First, the explanation must be consistent with the healing practice. On the medical side, the explanation is biological, and in psychotherapy the explanation is psychological. Second, the explanation must be acceptable and compatible with the patient’s attitudes, values, culture, and worldview. Third, the explanation must provide a strategy by which the patient can overcome difficulties and solve life’s problems. These three factors together make for a strong therapeutic alliance.
- The effective psychiatrist provides a treatment plan that is consistent with the explanation provided to the patient. Once the patient accepts the explanation, the treatment plan will make sense and patient compliance will be increased. The treatment plan must involve healthy actions—the effective psychiatrist promotes healing by replacing failed strategies with effective strategies. At the same time, strong defenses will replace weak defenses, and healthy practices will replace self-defeating behaviors.
- The effective psychiatrist is influential, persuasive, and convincing. The psychiatrist presents the explanation and the treatment plan in a way that convinces the patient that the explanation is correct and that following through with the treatment will benefit the patient. This process leads to patient hopefulness, increased expectancy for mastery, and healthy actions. These characteristics are essential for forming a strong working alliance.
- The effective psychiatrist is honest and authentic. Authenticity refers to communication to the patient that the psychiatrist truly wants to know how the patient is doing. The best psychiatrists tend not to use checklists, scales, and paper measures. Instead, they talk and listen openly and honestly.
- The effective psychiatrist is flexible and will be patient if resistance to the treatment is apparent or the patient is slow to make progress. Although the effective psychiatrist is persuasive, persuasion can be a process that takes time. The good psychiatrist pays attention, takes in new information, test hypotheses about the patient, and is willing to be wrong. A good psychiatrist will seek second opinions, refer to other specialists, and even take calculated risks such as trying a new approach or a newly released medication.
- The effective psychiatrist does not avoid difficult material in therapy. Doctor and patient must use such difficulties therapeutically. We all tend to avoid material that is difficult. The effective psychiatrist senses avoidance is taking place and does not collude to avoid the material. Instead, the psychiatrist will discuss the difficult material and address difficult problems. Sometimes conversations can be difficult, and at times the relationship between doctor and patient can be strained, but this is part of the work of therapy. The good psychiatrist can use skill, experience, and compassion to overcome these barriers to recovery.
- The effective psychiatrist communicates hope and optimism. Sometimes this is easy to do, and sometimes it’s difficult. The working partnership must maintain hope and optimism in the face of chronic illness, relapses, lack of consistent progress, and many other difficulties. Effective psychiatrists acknowledge these issues and still communicate hope that the patient will achieve realistic goals in the long run. This communication is not blind faith or Pollyanna optimism, but rather a firm belief that together the psychiatrist and patient will work successfully. At the same time, effective psychiatrists mobilize patient strengths and resources to facilitate the patient’s ability to solve his or her own problems. The best doctors know that the patient, through his or her work, is responsible for therapeutic progress, creating a sense of mastery.
- Effective psychiatrists are aware of the patient’s characteristics and context. This is a tall order with many categories: culture, race, ethnicity, spirituality, sexual orientation, age, physical health, motivation for change, and beyond. Furthermore, the effective psychiatrist is aware of how his own background, personality, and beliefs figure into the relationship.
- The effective psychiatrist is aware of his or her own psychological process and does not inject his or her own material into the therapy process unless such actions are deliberate and therapeutic.
- The effective psychiatrist is aware of the best research evidence related to the particular patient, in terms of treatment, problems, and social context. It is very important to understand the biological, social, and psychological basis of the patient’s problem.
- The effective psychiatrist seeks always to improve, always to be a student. Hippocrates said, “The life so short, the craft so long to learn,” and truer words were never spoken.
- Finally, the good psychiatrist must possess both humility and a sense of humor. We will never know enough, or be wise enough, to have all the answers. We cannot take ourselves too seriously, lest we become arrogant, prideful, and set ourselves apart from those who have graced us with the privilege of being socially sanctioned healers.
Development of skill in psychiatry involves intensive practice and unceasing professional growth. Patients are sometimes our best and most effective teachers. A few years ago I taught a seminar for third year students at the University of Texas Southwestern Medical School, “Psychiatric Nightmares, Disasters, and Catastrophes.” The entire content of the seminar consisted of mistakes I’d made, errors I had committed, and pitfalls that these students likely would encounter, sooner or later, in their medical careers.
I told the story of a patient with whom I’d had a terrible, angry argument, and how guilty I felt for years about my lack of composure—only to have the patient return, two years later, to ask me for a job at the hospital and tell me that she had been shaken into reality by our confrontation. I told them the story of the patient who overdosed and came to the ICU, and how I was baffled by the case—until I realized that the patient had diabetes, and was actually in a diabetic coma, not a drug-induced state.
I told them about the patient who came to the doorstep of my home on a Sunday afternoon, bearing in her arms her injured pet cat, hoping that I could help. I told them about an elderly man from New Orleans who was my patient in the middle of the night as Hurricane Katrina washed away his home.
And I told them about the time when I was called to the ER to examine a beautiful young woman, a Duke University cheerleader, who had bruised her shoulder. When I approached her to examine the injury, and she undid her gown and dropped it with a smile, I calmly reached into the pocket of my white coat for my stethoscope, only to realize that I then stuck my reflex hammer in my ear.
These encounters are the building blocks of the effective psychiatrist’s life. I’ve come to realize that most of the learning happens after we graduate. As Dr. Stead used to say at Duke, “Medical school is where you stay for four years until you’re old enough to become a doctor.”
Treatment Philosophy
My approach to psychiatric practice reflects many years studying human nature and working to help people who are having a hard time in life. By the time most people see a psychiatrist, they are worried, or they are sad, or they are very confused about something I will just call “the problem,” or “the complaint.” Let me make some general comments about my approach, and then I will discuss my thinking on the use of medications.

People seek psychiatric help for a variety of problems, but everyone wants the same result: to feel better, to think more clearly, to rediscover satisfaction and happiness, and to regain a sense of self control and personal freedom. The problem may be related to mood, energy level, motivation, sleep, worry, relationships, anger, troubled behavior, obsessions, compulsions -- it’s a long list. People who drink too much, use drugs, or misuse prescription medication are often using these chemicals to find relief. Alcoholism and substance abuse are widespread in our culture.
Dealing with life is never easy.
Most persons first try to solve the problem or deal with the complaint on their own. Frustrated that things aren’t improving, they may seek advice from others. Sometimes a person hides the problem or lives in silence with the complaint. They may read a book, go to a support group, consult the internet, or try a new religious practice. We all have problems and complaints, and we all do the best we can to solve the dilemmas of life. When someone calls me about consultation, I almost always hear them say that they have a problem, they have tried to solve the problem, and they are looking for someone who knows how to help make things better.
One of the individuals consulting with me said, “I feel like I’m in a box, and the directions for getting out of the box are printed -- on the outside of the box.”
A successful airline pilot, a Vietnam combat veteran, said, “Doc, I’m out of altitude, airspeed, and ideas.”
Often the person seeking help has waited so long that demoralization has begun to set in, and they are beginning to lose hope. This doesn’t mean that the individual is suicidal or, in fact, any more unhappy than many of the people at the workplace or in the neighborhood. It means that they are resigned to always feeling this way, never feeling any better than this. Demoralization means a state of mind in which a person considers accepting fate, giving up, and abandoning the idea that things can get better.
Fear, anger, resentment, feeling constantly wounded, feeling overwhelmed, feeling unappreciated, feeling worthless -- all of these emotions are part of our lives. But when we feel negative all the time, or most of the time, most days, then we need help. There are very few emotional problems that defy intelligent therapy and reasonable efforts toward a solution.
When I meet someone for the first time in consultation, I have three major concerns. First, I want to get to know the person and hear about the problem are the complaint. My first question usually is simply, “How can I help?” or “What brings you to see me?” Second, I want to explore the individual’s point of view or understanding of the problem, including what solutions have been attempted. Third, I want to consider what we can do, working together, to improve the situation. I tend to focus more on results than on reasons. I’m not always sure about why things happen, but I am very focused on what we can do now. Sometimes I explain in detail how the brain works, and sometimes I discuss how life works. The process of recovery involves growth, change, and even personal transformation.
Research shows that psychotherapy can help, medication can help, and intelligent problem solving helps. Psychotherapy is not for everyone, and medication is not for everyone, but the vast majority of people who want help can find it. One of my favorite expressions is, “You have to do it yourself, but you can’t do it alone.”
Over the years I have developed a style that I call “sober conversation.” The word “sober” does not apply just to alcohol and addictions. To be sober is to be serious, to focus on what is most important, and to try to get it right. I believe in the importance of what we care about, and in this regard I have seriously studied the specific problem of human will. I call it “the problem of human will” because we are often confused about what we will ourselves to do, or not to do. When I work as a psychotherapist, I am most interested in what people care about, how their beliefs and assumptions about life have been formed, and where they feel stuck or at odds with themselves. Sometimes we have conflicting feelings about the same thing. For example, someone wants to take life in a certain direction, but he or she feels conflicted about it. Or someone tries to solve a problem, not realizing that it’s part of a bigger problem, or a different kind of problem. My definition of psychotherapy is that it is a form of personal consultation, focused on the situation of the client, with the goal of solving problems and feeling better.

Not everyone is cut out for in-depth or long-term conversation. Some people like to come for a few visits, and some like to keep going for weeks, or even months on a weekly basis. Some people prefer to come two or three times a week because they want to do the work and get on with whatever is next. Some people come for an hour, and some come for an afternoon.
Psychotherapy does take time, because the process is basically two people getting to know each other in the context of a specific purpose. Psychotherapy at its best is about taking life seriously, getting it right, and feeling the satisfaction that comes from clarity of thought, commitment to integrity, and comfort with the complexity of one’s own emotions and ideas. Some say that psychotherapy is a dying art, and this may be true. Psychiatrists today (and perhaps psychologists as well) do not receive the extensive training in psychotherapy that we did thirty years ago. Many psychiatrists and psychologists are not interested in psychotherapy. And many psychotherapists are not really very good or very well trained. Today there are thousands of people who call themselves “life coaches,” and anyone can hang out a shingle and call himself a “life coach.” There are several private organizations that offer “certifications,” but there are no license requirements, there is no government regulation, and no educational standard that is generally accepted. For these reasons, I think the concept makes sense, but in practice let the buyer beware -- caveat emptor!
Medications can be very helpful in treating some specific psychiatric problems. Today we have excellent medications for anxiety, depression, moodswings, insomnia, attention deficit disorder, and other conditions. Bipolar disorder, for example, is a devastating condition that can be very effectively managed with medication, restoring individuals to a life of normalcy and stability. I have absolutely no doubt about the value of psychiatric medications. I also believe that what is most important is getting the right diagnosis and the correct strategy for intervention and treatment. I see many people who have been misdiagnosed, and even mistreated, because they have not been well assessed. Assessment can take time, and I never jump to conclusions about diagnosis. After knowing someone for a few weeks, together we may decide that we see the condition in a different way.
Psychiatric medications are powerful, effective tools when used properly, but they also have side-effects, and they are expensive. Getting the right medication for the right diagnosis is extremely important. And there is an old saying from Hippocrates, creator of The Hippocratic Oath: “It is more important to know what sort of person has a disease than to know what sort of disease a person has.“