Colleges Going to Pot?
INCREASE IN MARIJUANA USE
Between 2006 and 2014, use of any illicit drugs, including marijuana, fluctuated. In 2006, use of illicit drugs in the previous 12 months was at 34%, and then increased to 41% in 2013. In 2014, use decreased slightly, to 39%. The researchers noted that marijuana was the drug most driving this increase.
OTHER DRUGS
Illicit drug use in the previous 12 months that did not include marijuana also increased. In 2014, 21% of college students used illicit drugs, compared to only 15% in 2008, with the main increases being seen in amphetamine and ecstasy use, according to the study.
AMPHETAMINES, ADDERALL, RITALIN & RELATED DRUGS
The use of nonmedical amphetamines almost doubled from 2008 to 2012, and then slightly decreased by 2014, according to a press release. In the release, Johnston suggested that this increase in use could be attributed to students’ desire to improve their studies and test performance.
ECSTASY
Despite ecstasy use decreasing between 2004 and 2007, usage rose to 5.8% in 2012 from only 2.2% in 2007. A significant increase in use of cocaine within the past 12 months was also seen, rising from 2.7% in 2013 to 4.4% in 2014.
FAKE MARIJUANA, NARCOTICS, SALVIA
Use of synthetic marijuana, narcotic drugs and salvia decreased significantly by 2014. The researchers noted that use of bath salts was negligible among college students.
CIGARETTE SMOKING
Rates of cigarette use within the past 30 days decreased significantly among college students, dropping from 31% in 1999 to only 13% in 2014. Daily smoking also decreased significantly, from 19% in 1999 to only 5% in 2014.
HOOKAHS
However, while cigarette rates have dropped significantly, use of hookahs increased significantly to 33% in 2014, up from 26% in 2013. No significant change in cigar use was seen, according to the researchers.
ALCOHOL
In 2014, 63% of college students reported having had an alcoholic drink within the past 30 days, a decrease from 67% in 2000 and 82% in 1981. A decrease was also seen in the proportion of students reporting they had been drunk within the past 30 days, from 48% in 2006 to 43% in 2014. Rates of binge drinking, as defined by five or more drinks in a row within the previous 2 weeks, decreased from 44% in 1980 to 35% in 2014, among college students.
THE ORIGINAL REFERENCE ARTICLE (PDF File)
Johnston LD, et al. Monitoring the Future national survey results on drug use: 1975-2014: Volume 2, College students and adults aged 19-55. Ann Arbor: Institute for Social Research, The University of Michigan; 2014. http://www.monitoringthefuture.org/pubs/monographs/mtf-vol2_2014.pdf.
Painkiller Deaths Update
The study, led by Yih-Ing Hser, professor of psychiatry and behavioral sciences at the David Geffen School of Medicine at UCLA, is the first to look at the mortality rate of people with opioid use disorder in a general health care system rather than those treated at specialty addiction clinics. The mortality rate among patients in this setting, which includes primary care offices and large research hospitals, was more than two times higher than what previous studies had found in specialty clinics.
“The high rates of death among patients with opioid use disorder in a general health care system reported in this study suggest we need strategies to improve detection and treatment of this disorder in primary care settings,” Hser said.
Opioids often are prescribed to treat acute and chronic pain, and include prescription medications such as oxycodone (or OxyContin), hydrocodone (or Vicodin), codeine, morphine and fentanyl, as well as illicit substances such as heroin. The number of opioid overdoses in the United States has quadrupled since 1999, leading some physicians and policymakers to declare the opioid problem a national crisis. The 21st Century Cures Act, legislation signed in December by former President Barack Obama, included $1 billion in funding to help states address opioid abuse.
As rates of opioid addiction have risen, patients with opioid abuse problems increasingly are being treated by generalists, such as internists and primary care physicians, in doctors’ offices. Until now, researchers had not gauged the impact of this influx of patients with opioid abuse and addiction in primary care settings.
Hser and colleagues studied electronic health records, and an associated death index system, for 2,576 patients, ages 18 to 64, diagnosed with opioid use disorder from 2006 to 2014. The individuals received health care at a major university hospital system. While all of those studied had diagnoses of opioid use disorder, not all were receiving treatment for it.
By the end of the study period, 465 people (18.1 percent of the study population) had died. Based on how long each person had participated in the study — an average of about four years for each individual — the researchers calculated a crude mortality rate of 48.6 deaths per 1,000 person-years, more than two times higher than the 20.9 deaths per 1,000 reported in previous studies done in specialty addiction clinics. The rate was also more than 10 times higher than the expected death rate for people of the same age and sex in the general U.S. population.
Overall, the patients in the new study were older at diagnosis and had a higher rate of other diseases and disorders compared to patients included in previous studies that took place at specialty clinics. Hser’s team noted higher rates of both simultaneously occurring health complications — including hepatitis C, liver disease, cardiovascular disease, cancer and diabetes — as well as other substance abuse disorders involving tobacco, alcohol, cannabis and cocaine — among the patients who died.
“The findings were surprising because one would potentially expect better health care outcomes for patients being served by a large health care system,” Hser said. “Late identification of opioid use disorder and lack of addiction treatment could contribute to these high rates of serious health conditions and death.”
Black or uninsured individuals were also more likely to die during the study period, the researchers said, a finding they noted highlights the need for additional research on disparities in addiction care.
Additional research will be needed, they concluded, to determine how to best curb the mortality rates among all individuals with opioid use disorder and better integrate substance abuse disorder screening and treatment into primary care.
The study’s other authors are UCLA psychiatrists Larissa Mooney and Karen Miotto; UCLA professor of medicine Douglas Bell; UCLA graduate students Yuhui Zhu and Di Liang; David Huang, the senior statistician at the UCLA Integrated Substance Abuse Programs; and Andrew Saxon of the Veterans Affairs Puget Sound Health Care System.
The research was funded by the National Institute on Drug Abuse’s Clinical Trials Network.
http://newsroom.ucla.edu/releases/opioid-addiction-raises-mortality-rate
Painkillers: New Guidlines
Opioid painkillers such as OxyContin and Vicodin are now prescribed to as much as 4% of the U.S. population — 250 million prescriptions — with their use quadrupling since 1999. Some 1.9 million Americans are now addicted to, or dependent on, the painkillers. And from 1999 to 2014, about 165,000 people died of overdoses. Almost all of the opiate-related drugs on the market for pain are as addictive as heroin.
According to the National Institute on Drug Abuse (NIDA), the abuse of and addiction to opioids such as heroin, morphine, and prescription pain relievers is a serious global problem that affects the health, social, and economic welfare of all societies. It is estimated that between 26.4 million and 36 million people abuse opioids worldwide, with an estimated 2.1 million people in the United States suffering from substance use disorders related to prescription opioid pain relievers in 2012 and an estimated 467,000 addicted to heroin. The consequences of this abuse have been devastating and are on the rise. For example, the number of unintentional overdose deaths from prescription pain relievers has soared in the United States, more than quadrupling since 1999. There is also growing evidence to suggest a relationship between increased non-medical use of opioid analgesics and heroin abuse in the United States.
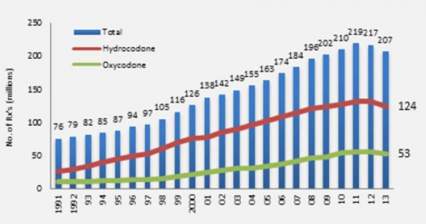
Increase in Opioid Prescriptions 1991-2013
Opioid medications can produce a sense of well-being and pleasure because these drugs affect brain regions involved in reward. People who abuse opioids may seek to intensify their experience by taking the drug in ways other than those prescribed. For example, extended-release oxycodone is designed to release slowly and steadily into the bloodstream after being taken orally in a pill; this minimizes the euphoric effects. People who abuse pills may crush them to snort or inject which not only increases the euphoria but also increases the risk for serious medical complications, such as respiratory arrest, coma, and addiction. When people tamper with long-acting or extended-release medicines, which typically contain higher doses because they are intended for release over long periods, the results can be particularly dangerous, as all of the medicine can be released at one time. Tampering with extended release and using by nasal, smoked, or intravenous routes produces risk both from the higher dose and from the quicker onset.
The Centers for Disease Control released a dozen opioid prescription guidelines in the Journal of the American Medical Association (JAMA). They will not have the power of law but will guide insurance company recommendations to doctors and Veterans Administration prescriptions for retired military patients, with the aim of curbing dangerous prescribing practices. "Primary care clinicians find managing chronic pain challenging," according to JAMA, and "evidence of long-term efficacy of opioids for chronic pain is limited. Opioid use is associated with serious risks, including opioid use disorder and overdose."
The guidelines are based on three principles. First, opioids should be a last option for these patients, with aspirin-related drugs and exercise preferred. Second, when given, doses should start out low and only increase slowly. Third, patients should be monitored and a plan for getting them off the drugs should start with their prescription. The guidelines also call for getting naloxone, a drug used to counteract overdoses, into the hands of more doctors, nurses, police, and emergency personnel.
Pain Pill Addiction: Basics
Breaking free of prescription drug abuse takes much more than willpower. As I often say, "You have to do it yourself, but you can't do it alone." There are individuals who claim to have "kicked" or achieved abstinence without any help, but I don't know many of them. Early on, before dependency sets in, it's possible to recognize the problem and stop using narcotics. Once dependence sets in, though, it's not so easy.
Fortunately, medications and counseling can improve the chances of success. Newer drugs like buprenorphine (sometimes combined with naloxone) and naltrexone and traditional therapies like methadone and 12-step programs, are helping thousands of people stay on the road to recovery.
Physical Dependence and Detoxification
Narcotic addiction leads to real changes in certain areas of the brain. Prescription drug addiction alters the circuits responsible for mood and "reward" behaviors.
In addition, long-term prescription drug abuse affects virtually all the systems in the body. Cutting off the supply abruptly leads to opioid withdrawal symptoms.
Symptoms of opioid withdrawal include:
- Craving for drugs
- Diarrhea
- Large pupils
- Yawning
- Abdominal pain
- Chills and goose bumps (the origin of the phrase "cold turkey")
- Nausea and vomiting
- Body aches
- Agitation and severe negative moods
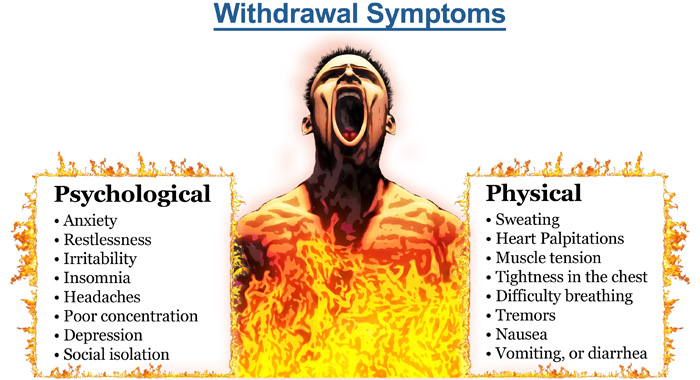
A list of symptoms doesn't capture the agony of opioid withdrawal.
The syndrome is intensely unpleasant, and people will do almost anything to avoid it.
Opioid withdrawal lasts from hours to several days -- and sometimes weeks -- depending on how long and how much a person has used their drug of choice. After the intense initial symptoms subside, some physical and mental discomfort may persist for weeks.
Medications for Opioid Withdrawal
Opioid withdrawal is difficult to endure, and is a major reason for relapse and continued prescription drug abuse. Medications are used to prevent symptoms of opioid withdrawal during detox, easing the person out of physical dependence:
Methadone is a long-acting opioid drug. It activates the same opioid receptors as narcotics, effectively eliminating withdrawal symptoms. Providing the correct dose of methadone prevents opioid withdrawal symptoms and eases drug craving but it does not provide the euphoria. The dose can be slowly tapered off, freeing the person from physical dependence without withdrawal symptoms. Methadone is the most effective known treatment for narcotic addiction.
Buprenorphine and Naloxone (Suboxone) is a newer combination drug that helps for detox from prescription opioid addiction. Buprenorphine activates opioid receptors, reducing drug craving and preventing withdrawal. Naloxone helps prevent misuse of the medication.
Clonidine is a blood pressure medicine that acts on the brain. Clonidine reduces the effects of the "fight or flight" response, which is over-activated during opioid withdrawal. However, clonidine does nothing to reduce drug craving, and is mostly ineffective when used alone.
"Rapid detox" programs claim to accelerate the process of detox and opioid withdrawal by giving large doses of opioid blocking drugs. Some programs place an addict under general anesthesia during the detox process. These programs have not proven to be more effective than traditional methods of detox, and may be more dangerous.
Maintenance Therapy After Detox
Completing detox subdues the physical effects of narcotic addiction and opioid withdrawal. But experts say psychological and social factors are the main drivers that push addicts back to using. Stress and situations that remind the brain of the drug's pleasure are common triggers.
When drug cravings strike, they can be impossible to resist. Most people who go through detox and short-term counseling will relapse to prescription drug abuse.
Studies show that the chances of beating narcotic addiction are better with long-term maintenance therapy with either methadone or buprenorphine paired with naloxone (Zubsolv, Bunavail, Suboxone) . These drugs are used during the maintenance phase of treatment. People on these drugs are still opioid-dependent, but they are often freed from their destructive drug addiction. They can return to work, drive without impairment, and function normally in society. Naloxone has also been combined with oxycontin ( Targiniq ER ) to deter abuse by snorting or injecting the drug. A person can still become addicted by taking it orally, however.
Methadone is the best-studied, most effective method of recovery from narcotic addiction. Suboxone, while newer, has gained wide acceptance as maintenance therapy.
Some people have a high rate of relapse when maintenance therapy is stopped, and so they remain on the medicines for decades. In others, maintenance therapy is tapered off over months to years.
Naltrexone (ReVia, Vivitrol) is an opiate receptor-blocking medication used in maintenance therapy for narcotic addiction. Unlike methadone and Suboxone, naltrexone does not activate receptors at all, so it does not reduce opioid withdrawal or craving. However, because naltrexone blocks opiate receptors, a person won't get high if he or she uses drugs while taking the medicine. The drug is usually ineffective by itself, because people can simply stop taking it and get high shortly after.
Counseling and 12-Step Programs
Narcotics Anonymous (NA) is an international network of community-based meetings for those recovering from drug addiction. Modeled after Alcoholics Anonymous (AA), NA is a 12-step program with a defined process for overcoming narcotic addiction.
NA is an abstinence-based program. In principle, NA is opposed to the use of maintenance therapy. Methadone Anonymous is a 12-step program that acknowledges the value of methadone or Suboxone in recovery from narcotic addiction. Methadone Anonymous has caught on in California, but I don't know much about meetings in Texas. If you have information about Methadone Anonymous meetings, contact me.
Most of us who are experts in the field recommend participation in a 12-step program or other form of counseling. Therapy can take place as an outpatient, or in a residential facility. I discuss the value of 12 Step Programs on my FAQ page.
Update on Marijuana Research
According to a recent analysis presented at the 2015 Meeting of the American Chemical Society, the amount of THC in samples from marijuana sold in Colorado are reaching 30 percent. Three major patterns have emerged over the past few months since Andy LaFrate, Ph.D., and his lab began testing marijuana samples. Those patterns concern potency, amounts of a substance called CBD and contaminants in the products.
“As far as potency goes, it’s been surprising how strong a lot of the marijuana is,” LaFrate says. “We’ve seen potency values close to 30 percent THC, which is huge.” LaFrate is the president and director of research of Charas Scientific, one of eight labs certified by Colorado to do potency testing.
THC is an abbreviation for tetrahydrocannabinol, which is the psychoactive compound in the plant. He explains that three decades ago, THC levels were well below 10 percent. Its content has tripled in some strains because producers have been cross-breeding them over the years to meet user demands for higher potency, he says.
But an unexpected consequence of this breeding has occurred, says LaFrate. Many of the samples his lab has tested have little to no cannabidiol, or CBD. CBD is a lesser known compound in marijuana that is of increasing interest to medical marijuana proponents. Researchers are investigating CBD as a treatment for schizophrenia, Huntington’s disease and Alzheimer’s disease. It is also being considered for anxiety and depression. But unlike THC, CBD doesn’t get people high — that’s a key trait for many people who are wary of buzz-inducing drugs and for potential medical treatments for children. As for recreational users, the lack of CBD in marijuana means that many of the hundreds of strains they select from could in actuality be very similar chemically, according to LaFrate.
"What we have today is not the weed we used to smoke in the 1960's."
In a recent report researchers found that the concentration of THC sold on the streets in Denmark has tripled to an average of 28 percent in the last 20 years.
Attitudes toward marijuana are also rapidly changing. In the 1960s surveys found a mere 12 percent supported marijuana legalization—now, more than 50 percent are in favor. Over the past decade recreational/medicinal use of cannabis was legalized in the District of Columbia as well as in Alaska, Colorado, Oregon and Washington State; 19 other states also permit the use of the drug for medical purposes. As more states and countries, such as Canada and the U.K., consider following suit, advocates and critics are engaging in heated debates about the potential risks and rewards—particularly in light of the increasing prevalence of highly potent marijuana. But the evidence is nebulous—even within the scientific community, there is lack of consensus about how much harm marijuana can do to users’ brains and mental health.
In addition to THC, the other major component of marijuana that has caught the attention of researchers is cannabidiol (CBD), which scientists have linked to antipsychotic properties. Not only do THC and CBD have opposing effects, cannabis with higher THC content tends to contain lower amounts of CBD. “The relationship between CBD and THC is unique, in that the biological process required to make THC antagonizes the generation of CBD,” says Matthew Hill, a cannabinoid neuropharmacologist at the University of Calgary.
Damage to the brain?
In an article published last month in Psychological Medicine, researchers conducted a neuroimaging study to assess the effects of cannabis use on the corpus callosum, the largest collection of white matter in the brain containing fibers that facilitate communication between the two hemispheres. They found that this structure was negatively affected in those who used high potency cannabis—strains high in THC and low in CBD—compared with those who used lower strength bud or did not use at all. Moreover, the changes were similar in both those with and without previous episodes of psychosis. However, the researchers assert that they did take other drug usage into account.
Previous studies have demonstrated the importance of these confounding factors when interpreting marijuana’s effects on the brain. For example, a 2014 study in The Journal of Neuroscience reported that marijuana use was associated with changes in brain structures associated with reward processing. This effect was dose-dependent, meaning the more cannabis someone used, the more changes became apparent in their brains. In a subsequent study, published in 2015 in the same journal, another group of researchers found that once variables such as alcohol use, gender and age were controlled for, the differences between users and nonusers disappeared.
Marijuana madness?
In a study published earlier this year in Lancet Psychiatry the same group of researchers at King’s College found that using cannabis, and THC specifically, can produce acute psychotic symptoms, and some researchers suggest it increases the risk of developing schizophrenia. The link between marijuana and psychosis, however, has been a matter of heated debate in the scientific community. Researchers have argued that there are sufficient grounds to doubt the causality of this link. There are two alternative possibilities: being predisposed to schizophrenia may increase the likelihood for cannabis use or a third variable may make it more likely for people to use marijuana and develop schizophrenia. For example, previous studies have suggested that schizophrenia and cannabis share both genetic and demographic risk factors, such as low socioeconomic status.
Critics also point to the fact that all the studies to date have been correlational. But this does not immediately dismiss the possibility that causation is possible. After all, although there was a strong correlational link between smoking and cancer, it took a study of more than 30,000 British doctors to confirm causality.
According to Haney, the odds ratio—the likelihood that an exposure will lead to a certain outcome—of marijuana causing psychosis are much lower than those for smoking and cancer. “There is also an association with tobacco smoking and schizophrenia that is much stronger [than cannabis use],” Haney says. “If this relationship is causal, it is a tiny effect, which might explain why there hasn't been a dramatic upsweep in rates of schizophrenia in recent years.”
Both Haney and Evins agree that it is biologically plausible that marijuana, particularly at a young age, could increase the likelihood of negative psychiatric outcomes. The developing brain has an abundance of cannabinoid type 1 (CB1) receptors, where THC binds to exert its effects, in the prefrontal cortex, a key brain area impacted by schizophrenia. “I don't think it's a good idea for young children to be smoking marijuana at all because of their developing brains but I am extremely cautious about pinning it all on marijuana when there is a potential for many other explanations,” Haney says.
To truly determine whether marijuana causes such effects, scientists would need to track changes that occur in a large number of individuals before and after they use a drug over a long period of time. An effort to conduct this type of study is currently underway—the National Institutes of Health recently funded the multicenter Adolescent Brain Cognitive Development Study, which plans to recruit 10,000 children before they start drug use, and follow them for 10 years to assess the short-and long-term effects of using marijuana, tobacco and other drugs.
Teenagers and young adults at risk?
Cannabis has been found to impair cognitive functions such as memory and is increasingly being considered an addictive substance, especially in adolescents. There are still many questions that remain to be answered but strict regulation and lack of funding pose large barriers to conducting the required studies. The U.S. Drug Enforcement Administration still classifies marijuana in its most restrictive “Schedule I” category, which puts tight regulations on researchers who want to study its effects.
A New Zealand study found that persistent cannabis users show neuropsychological decline from childhood to midlife. These scientists found that frequent and persistent marijuana use starting in adolescence was associated with a loss of an average of 8 IQ points measured in mid-adulthood. Significantly, in that study, those who used marijuana heavily as teenagers and quit using as adults did not recover the lost IQ points.
Users who only began using marijuana heavily in adulthood did not lose IQ points. These results suggest that marijuana has its strongest long-term impact on young users whose brains are still busy building new connections and maturing in other ways. The endocannabinoid system is known to play an important role in the proper formation of synapses (the connections between neurons) during early brain development, and a similar role has been proposed for the refinement of neural connections during adolescence. If confirmed by future research, this may be one avenue by which marijuana use during adolescence produces its long-term effects. (For details see: Meier MH, Caspi A, Ambler A, et al. Persistent cannabis users show neuropsychological decline from childhood to midlife. Proc Natl Acad Sci USA. 2012;109:E2657-2664.)
The ability to draw definitive conclusions about marijuana’s long-term impact on the human brain from past studies is often limited by the fact that study participants use multiple substances, and there is often limited data about the participants’ health or mental functioning prior to the study. Over the next decade, the National Institutes of Health is planning to fund a major longitudinal study that will track a large sample of young Americans from late childhood (before first use of drugs) to early adulthood. The study will use neuroimaging and other advanced tools to clarify precisely how and to what extent marijuana and other substances, alone and in combination, affect adolescent brain development.
Scientists agree the highly potent marijuana may be better to avoid. Aside from potential long-term harm, receiving a high dose of THC can be especially risky for first-time users who are more likely to experience adverse effects such as panic or anxiety attacks. But even knowing the potency of a product, consumers might not always get what they ask for.
Because of competing laws at the state and federal level, the quality of regulation varies largely between states and regions. Although THC potency labeling is mostly required for both medical and recreational products, it is not always accurate—a study published this June in JAMA The Journal of the American Medical Association revealed that of the 75 edible marijuana products (from 47 different brands) researchers assessed only 17 percent accurately labeled their THC content.
The article states: "Edible cannabis products from 3 major metropolitan areas, though unregulated, failed to meet basic label accuracy standards for pharmaceuticals. Greater than 50% of products evaluated had significantly less cannabinoid content than labeled, with some products containing negligible amounts of THC. Such products may not produce the desired medical benefit.
"Other products contained significantly more THC than labeled, placing patients at risk of experiencing adverse effects.5,6 Because medical cannabis is recommended for specific health conditions, regulation and quality assurance are needed.
"A limited number of cities, dispensaries, and products were included. Because no source lists all dispensaries, and many products are not labeled with cannabinoid content, a true random sample was not possible and the results may not be generalizable. However, this study illustrates the variability in label accuracy for edible cannabis products within 2 of the largest medical cannabis markets in the United States."
Across labs and in homes, marijuana remains a highly debated issue. Marijuana is an extremely polarizing topic among scientists, as these articles demonstrate. My own view is that marijuana is not likely to cause someone to suffer a schizophrenic illness, but clearly what we have today is not the weed we smoked in the 1960's.
CASA Report on Addictions
CASA Columbia’s work for this report involved:
• A review of more than 7,000 publications
• Analyses of 5 national data sets
• Interviews with and suggestions from 176 leading experts in a broad range of fields relevant to the report
• Focus groups and a national general population survey of 1,303 adults about their attitudes and beliefs related to addiction and its treatment
• Two New York State surveys of addiction treatment providers
• An online survey of 1,142 members of professional associations involved in addiction care
• An online survey of 360 individuals with a history of addiction
• Analyses of state and federal governments’ and professional associations’ licensing and certification requirements for treatment providers
• A case study of addiction treatment in New York State and New York City
This 5-year study found that, despite the prevalence of addiction, the enormity of its consequences, the availability of effective solutions and the evidence that addiction is a disease, both screening and early intervention for risky substance use are rare, and only about 1 in 10 people with addiction involving alcohol or drugs other than nicotine receive any form of treatment.
Of those who do receive treatment, few receive anything that approximates evidence-based care. This compares with 70% to 80% of people with such diseases as high blood pressure and diabetes who do receive treatment. This report exposes the fact that most medical professionals who should be providing addiction treatment are not sufficiently trained to diagnose or treat the disease, and most of those providing addiction care are not medical professionals and are not equipped with the knowledge, skills or credentials necessary to provide the full range of effective treatments. Misunderstandings about the nature of addiction and the best ways to address it, as well as the disconnection of addiction medicine from mainstream medical practice, have undermined effective addiction treatment.
CASA Recommendations: The time has come for addiction medicine to be fully integrated into health care systems and medical practice. Health care providers, especially physicians, are our front line in disease prevention and treatment. They must understand the risk factors for addiction, screen for risky substance use and intervene when needed, and diagnose, treat and manage addiction just as they do all other diseases.
Other health care providers, including nurse practitioners, physician assistants, psychologists and social workers, are critical parts of the solution as well. We need national, evidence-based standards that stipulate who may provide addiction treatment, and core competencies for all health care providers integrated into their education and licensing requirements. We must regulate addiction treatment facilities and programs as health care providers and hold them accountable for treatment consistent with medical standards and proven practices.
Never Underestimate the Power of a Single Intervention
A few minutes of counseling in a primary care setting could go a long way toward steering people away from risky drug use -- and possibly full-fledged addiction, a UCLA-led study suggests. (Primary care refers to family physicians and other non-psychiatrists who provide most of our medical care.)
People who participated in the Quit Using Drugs Intervention Trial, or Project QUIT, which was a randomized controlled trial conducted in medical clinics, reduced their risky drug use by one-third when primary care doctors and health coaches provided them with brief interventions during a routine visit and follow-up phone calls.
Risky drug use is defined as the casual, frequent or binge use of illicit drugs such as cocaine, heroin and methamphetamine, or the misuse of prescription medications, without showing physiological or psychological signs of addiction. There are an estimated 68 million such drug users in the United States. These people are at risk not only for becoming addicts, but suffering attendant physical, mental health and social problems.
The study, published today in the peer-reviewed journal Addiction, is the first to demonstrate that a brief intervention led by a primary care physician can significantly reduce risky drug use among patients.
We Don't Plan to Become Addicts or Alcoholics
Most of the patients I (Dr. Talmadge) see in practice did not plan to become addicted to drugs. Casual use introduces powerful chemicals in the brain, and many of us then have our brains hijacked by these chemicals. As described in the HBO special on addictions, the human brain is an extraordinarily complex and fine-tuned communications network containing billions of specialized cells (neurons) that give origin to our thoughts, emotions, perceptions and drives. Often, a drug is taken the first time by choice to feel pleasure or to relieve depression or stress. But this notion of choice is short-lived. Why? Because repeated drug use disrupts well-balanced systems in the human brain in ways that persist, eventually replacing a person's normal needs and desires with a one-track mission to seek and use drugs. At this point, normal desires and motives will have a hard time competing with the desire to take a drug.
How Does the Brain Become Addicted?
As described in the HBO documentary, typically it happens like this:
-A person takes a drug of abuse, be it marijuana or cocaine or even alcohol, activating the same brain circuits as do behaviors linked to survival, such as eating, bonding and sex. The drug causes a surge in levels of a brain chemical called dopamine, which results in feelings of pleasure. The brain remembers this pleasure and wants it repeated.
-Just as food is linked to survival in day-to-day living, drugs begin to take on the same significance for the addict. The need to obtain and take drugs becomes more important than any other need, including truly vital behaviors like eating. The addict no longer seeks the drug for pleasure, but for relieving distress.
-Eventually, the drive to seek and use the drug is all that matters, despite devastating consequences.
-Finally, control and choice and everything that once held value in a person's life, such as family, job and community, are lost to the disease of addiction.
What brain changes are responsible for such a dramatic shift?
Research on addiction is helping us find out just how drugs change the way the brain works. These changes include the following:
Reduced dopamine activity. We depend on our brain's ability to release dopamine in order to experience pleasure and to motivate our responses to the natural rewards of everyday life, such as the sight or smell of food. Drugs produce very large and rapid dopamine surges and the brain responds by reducing normal dopamine activity. Eventually, the disrupted dopamine system renders the addict incapable of feeling any pleasure even from the drugs they seek to feed their addiction.
Altered brain regions that control decisionmaking and judgment. Drugs of abuse affect the regions of the brain that help us control our desires and emotions. The resulting lack of control leads addicted people to compulsively pursue drugs, even when the drugs have lost their power to reward.
The disease of addiction can develop in people despite their best intentions or strength of character. Drug addiction is insidious because it affects the very brain areas that people need to "think straight," apply good judgment and make good decisions for their lives. No one wants to grow up to be a drug addict, after all.
The addiction study cited above has some limitations. The results are based on participants' self-reporting, so the study may suffer from reporting bias. However, researchers found that based on urine testing, under-reporting of drug use was low. Additional limitations: not everyone in the clinic waiting rooms agreed to participate, which could impact the study's generalizability; there was some attrition during the study, though the 75 percent participation rate at follow-up compares to other studies of low income patients and drug use; and the three month follow up was relatively short.
There is a need for larger trials to gauge the QUIT program's effectiveness, but based on these findings the project appears to have the potential to fill an important gap in care for patients who use drugs, particularly in low-income communities, Gelberg said.
Read the entire report and article by clicking here.
News Flash! Interesting Articles...
Should a Worker Be Fired for Using Medical Marijuana at Home? Healthline , By R. Sam Barclay, July 9, 2015 Advocates Push to Expand Use of Medications to Treat Addiction USA Today , By Liz Szabo, July 8, 2015 Virtual Reality Shows How Dangerous it is to Drive Drunk and Stoned PBS NewsHour , By Catherine Woods, June 27, 2015 Neuroscience: Rewiring the Brain Nature , By Katherine Bourzac, June 25, 2015 Genetics: No More Addictive Personality Nature , By Maia Szalavitz, June 24, 2015 "Pharmacotherapy: Quest for the Quitting Pill" Nature , By Cassandra Willyard, June 24, 2015 Study Analyzes How Much Pot Impairs Drivers USA Today , By Trevor Hughes, June 23, 2015 "How Much Does Marijuana Impact Your Driving?" TIME , By Eliza Gray, June 23, 2015 "Designer Drugs Hit Dangerous Lows to Bring New Highs" Science News , By Kate Baggaley, May 05, 2015
Drug Overdose Deaths, Injuries
The good news? We are better off than 38 other states when it comes to events like drug overdose, car wrecks, killings, drownings, and the million other ways to die in The West. I just reviewed the report sponsored by the Robert Wood Johnson Foundation, a leading source of funding for medical research and education.
In The Facts Hurt: A State-By-State Injury Prevention Policy Report, Texas ranked 39th highest for the number of injury-related deaths in the state, with a rate of 55.3 per 100,000 people. Overall, the national rate is 58.4 per 100,000.
Rates in Texas decreased over the past four years for injury deaths, which includes drug overdoses, motor vehicle crashes, homicides and others. Overall, 17 states increased, 24 remained stable and 9 decreased. Injuries are the leading cause of death for Americans ages 1 to 44 – and are responsible for nearly 193,000 deaths per year.
Drug overdoses have become the leading cause of injury in 36 states, not including Texas, surpassing motor vehicle-related deaths.
Some key findings include:
Drug abuse: More than 2 million Americans misuse prescription drugs. The prescription drug epidemic is also contributing to an increase in heroin use; the number of new heroin users has doubled in the past seven years.
Key report indicators include the finding that 34 states and Washington, D.C. have “rescue drug” laws in place to expand access to, and use of naloxone - a prescription drug that can be effective in counteracting an overdose - by lay administrators. This is double the number of states with these laws in 2013 (17 and Washington, DC). While every state except Missouri has some form of Prescription Drug Monitoring Program (PDMP) in place to help reduce doctor shopping and bad prescribing, only half (25) require mandatory use by healthcare providers in at least some circumstances.
Motor vehicle deaths: Rates have declined 25 percent in the past decade (to 33,000 per year).
Key report indicators include observation that 21 states have drunk driving laws that require ignition interlocks for all offenders;
and while most states have Graduated Drivers Licenses that restrict times when teens can drive, 10 states restrict nighttime driving for teens starting at 10 pm; and 35 states and Washington, D.C. require car safety or booster seats for children up to age 8.
Homicides: Rates have dropped 42 percent in the past 20 years (to 16,000 per year).
The rate of Black male youth (ages 10 to 24) homicide victims is 10 times higher than for the overall population. One in three female homicide victims is killed by an intimate partner. Research shows that 31 states have homicide rates at or below the national goal of 5.5 per every 100,000 people.
Suicides: Rates have remained stable for the past 20 years (41,000 per year). More than one million adults attempt suicide and 17 percent of teens seriously consider suicide each year. Seventy percent of suicides deaths are among White males.
Falls: One in three Americans over the age of 64 experiences a serious fall each year, falls are the most common nonfatal injuries, and the number of fall injuries and deaths are expected to increase as the Baby Boomer cohort ages.
A key report indicator includes: 13 states have unintentional fall-related death rates under the national goal (of 7.2 per 100,000 people – unintentional falls).
Traumatic brain injuries: (TBIs) from sports/recreation among children have increased by 60 percent in the past decade.
Nationally, drug overdose deaths have more than doubled in the past 14 years – resulting in 44,000 deaths per year, and half of those deaths (22,000) are related to prescription drugs. Texas ranked sixth lowest for drug overdose deaths—at a rate of 9.6 per 100,000 people.
Texas scored three out of 10 on key indicators of steps states can take to prevent injuries – nationally, 29 states and Washington, D.C. scored a five or lower. New York received the highest score of nine out of a possible 10 points, while four states scored the lowest, Florida, Iowa, Missouri and Montana, with two out of 10 points.
Drug overdoses are the leading cause of injury deaths in the United States, at nearly 44,000 per year. Prescription drugs are the leading cause.
These deaths have more than doubled in the past 14 years, and half of them are related to prescription drugs (22,000 per year). Overdose deaths now exceed motor vehicle-related deaths in 36 states and Washington, D.C. And, in the past four years, drug overdose death rates have significantly increased in 26 states and Washington, D.C. and decreased in six.
The Facts Hurt report uses10 key indicators of leading evidence-based strategies that help reduce injuries and violence. The indicators were developed in consultation with top injury prevention experts from the Safe States Alliance and the Society for the Advancement of Violence and Injury Research (SAVIR).
The 10 indicators include:
▪ Does the state have a primary seat belt law? (34 states and Washington, D.C. meet the indicator and 16 states do not.)
▪ Does the state require mandatory ignition interlocks for all convicted drunk drivers, even first-time offenders? (21 states meet the indicator and 29 states and Washington, D.C. do not.)
▪ Does the state require car seats or booster seats for children up to at least the age of 8? (35 states and Washington, D.C. meet the indicator and 15 do not.)
▪ Does the state have Graduated Driver Licensing laws - restricting driving for teens starting at 10 pm? (11 states meet the indicator and 39 states and Washington, D.C. do not. Note a number of other states have restrictions starting at 11 pm or 12 pm.)
▪ Does the state require bicycle helmets for all children? (21 states and Washington, D.C. meet the indicator and 29 states do not.)
▪ Does the state have fewer homicides than the national goal of 5.5 per 100,000 people established by the U.S. Department of Health and Human Services (HHS) (2011-2013 data)? (31 states meet the indicator and 19 states and Washington, D.C. do not.)
▪ Does the state have a child abuse and neglect victimization rate at or below the national rate of 9.1 per 1,000 children (2013 data)? (25 states meet the indicator and 25 states and Washington, D.C. do not.)
▪ Does the state have fewer deaths from unintentional falls than the national goal of 7.2 per 100,000 people established by HHS (2011-2013 data)? (13 states meet the indicator and 37 states and Washington, D.C. do not.)
▪ Does the state require mandatory use of data from the prescription drug monitoring program by at least some healthcare providers? (25 states meet the indicator and 25 states and Washington, D.C. do not.)
▪ Does the state have laws in place to expand access to, and use of, naloxone, an overdose rescue drug by laypersons? (34 states and D.C. meet the indicator and 16 states do not.)
Score Summary: Texas Scores 3 out of 10
For the state-by-state scoring, states received one point for achieving an indicator or zero points if they did not achieve the indicator. Zero is the lowest possible overall score, 10 is the highest.
9 out of 10: New York
8 out of 10: Delaware
7 out of 10: California, New Jersey, North Carolina, Tennessee, Washington and West Virginia
6 out of 10: Alaska, Colorado, Hawaii, Indiana, Kentucky, Louisiana, Maine, Minnesota, Nevada, New Mexico, Oregon, Rhode Island and Virginia
5 out of 10: Alabama, Arkansas, Connecticut, Georgia, Illinois, Kansas, Massachusetts, Oklahoma, Utah, Vermont and Wisconsin
4 out of 10: Arizona, District of Columbia, Idaho, Maryland, Michigan, Mississippi, New Hampshire, North Dakota and Pennsylvania
3 out of 10: Nebraska, Ohio, South Carolina, South Dakota, Texas and Wyoming
2 out of 10: Florida, Iowa, Missouri and Montana
Painkiller Overdoses On the Rise
This news isn’t shocking to those of us who encounter addiction daily, but it’s in the headline today at USA Today. Other items of note from today’s paper:
With nearly 44,000 deaths a year, more Americans today die from drug overdoses than from car accidents or any other type of injury. Many of these deaths could be prevented if patients had better access to substance abuse therapy, experts say. Yet people battling addiction say that treatment often is unavailable or unaffordable.
Only 11% of the 22.7 million Americans who needed drug or alcohol treatment in 2013 actually got it, according to the Substance Abuse and Mental Health Services Administration. While some of those who went without care did so by choice, at least 316,000 tried and failed to get treatment.
"We know addiction treatment saves lives, reduces drug use, reduces criminal activity and improves employment," says Paul Samuels, president and director of the Legal Action Center, which advocates on behalf of people with HIV or addiction. "The data is there, the evidence is in, but our public policy has not caught up with the science."
Meanwhile, the crisis is getting worse, says Thomas Frieden, director of the Centers for Disease Control and Prevention. The death rate from drug overdoses more than doubled from 1999 to 2013, according to the CDC. The bulk of these deaths involve opiates, a class of pain killers that includes morphine and Oxycontin.
Injection drug use has fueled an outbreak of HIV in rural Indiana, a nationwide surge in hepatitis C infections, and an increase in the number of babies born addicted to drugs. States have responded to the surge in overdose deaths by expanding access to naloxone, a fast-acting rescue drug that can reverse the effects of an opiate overdose. Indiana lawmakers also voted to allow needle exchange programs in communities facing a public health crisis related to injection drug use. While those approaches are welcome, they don't treat the underlying addiction.
The wait for a spot in a detoxification program ranges from days to weeks, and it can be very expensive. As I say elsewhere here on my site, it's also true that not all treatment is really good treatment. Consumers are disadvantaged twice. Not only is treatment hard to find in the first place, but it's hard to know what constitutes a good treatment program. I have some comments about this on my FAQ page and on my Philosophy page.
Kevin McCauley, M.D. on Addiction
Best Therapists = Best Outcomes (by far)
Treatment: Know What to Ask
SEEKING TREATMENT: KNOW WHAT TO ASK
My goal in helping people includes educating them about what questions to ask.
Finding the right treatment for a person’s specific needs is critical. And finding the right treatment is not easy. Drug and alcohol addiction treatment is not “one size fits all.”
Treatment outcomes depend upon:
- the extent and nature of the person’s problems;
• the appropriateness of treatment; - the competence and skill of clinical staff;
• the availability of additional services; and
• the quality of interaction between the person and the treatment providers.
Family and friends play important roles in motivating people with drug problems to enter and remain in treatment. However, trying to identify the right treatment programs for a loved one can be a difficult process.
The National Institute on Drug Abuse (NIDA) has sound advice about the five questions to ask when searching for a treatment program:
1. Does the program use treatments backed by scientific evidence?
In the internet era, answering this question has become increasingly difficult. Many programs offer flashy "treatments" that are not scientific at all, despite claims made on beautiful web pages. According to Thomas McLellen, professor of psychiatry at the University of Pennsylvania, 90% of patients who enter addiction treatment programs don’t receive evidence-based treatment. Many current programs actually reject scientific evidence. For example, they prohibit the use of addiction medications, even though they’ve been shown to be more effective treating some addictions (specifically, the range of opiates like Oxycontin to heroin) than anything else. My concern is a bit different from Dr. McLellan's view (for example, he is not friendly toward 12 Step work). My major concern is that there are dozens of quack therapies, ranging from nutritional "cures" to "new age" approaches, to potentially harmful "trauma therapy."
A great website is not a guarantee that the advertised program is any good at all. Many programs today, using clever marketing, take advantage of opposition to Alcoholics Anonymous and 12 Step Programs by advertising that says, "We are NOT a 12 Step Program!" What these programs fail to do, in almost every example, is to state clearly what they actually do in their approach. Many other websites—and I have reviewed hundreds of them—claim to offer "evidence based treatment," when in fact the program is not evidence based at all. The average person has no idea whether or not claims of scientific evidence are true. Above all, beware of "testimonials" and celebrity endorsements. In selecting a treatment program, you have to use at least as much good judgment as you would use if you were buying a new car or having heart surgery.
Effective alcoholism and addiction treatments can include cognitive behavioral therapy, medications, or, ideally, the combination of both.
Key elements include:
• addressing a patient’s motivation to change;
• providing incentives to stop drinking or using drugs;
• building skills to resist alcohol/drug use;
• replacing addiction related activities with constructive and rewarding activities;
• improving problem-solving skills; and
• building better personal relationships.
Any and every good addiction treatment program will include competent assessment by a qualified addiction psychiatrist. Some programs will team an addiction medicine doctor with a well-qualified clinical psychologist, and that can work well. The point is that everything begins with getting the right assessment. Medications are an important part of treatment for many patients, especially when combined with counseling and other behavioral therapies. Different types of medications may be useful at different stages of treatment: to stop alcohol and drug abuse, to stay in treatment, and to avoid relapse.
2. Does the program tailor treatment to the needs of each patient?
No single treatment is right for everyone. The best treatment addresses a person’s various needs, not just his or her alcohol and drug abuse. Matching treatment settings, programs, and services to a person’s unique problems and level of need is key to his or her ultimate success in returning to a productive life. It is important for the treatment approach to be broad in scope, taking into account a person’s age, gender, ethnicity, and culture. The severity of addiction and previous efforts to stop using drugs can also influence a treatment approach.
The best programs provide a combination of therapies and other services to meet a patient’s needs. In addition to addiction treatment, a patient may require other medical services, family therapy, parenting support, job training, and social and legal services.
Finally, because addictive disorders and other mental disorders often occur together, a person with one of these conditions should be assessed for the other. And when these problems co-occur, treatment should address both (or all conditions), including use of medications, as appropriate.
Medical detoxification is a necessary first step in the treatment of certain addictions, but by itself does little to change long-term drug use.
3. Does the program adapt treatment as the patient’s needs change?
Individual treatment and service plans must be assessed and modified as needed to meet changing needs.
A person in treatment may require varying combinations of services during its course, including ongoing assessment. For instance, the program should build in drug monitoring so the treatment plan can be adjusted if relapse occurs. For most people, a continuing care approach provides the best results, with treatment level adapted to a person’s changing needs. A patient’s needs for support services, such as day care or transportation, should also be met during treatment.
4. Is the duration of treatment sufficient?
Remaining in treatment for the right period of time is critical. Appropriate time in treatment depends on the type and degree of a person’s problems and needs. People argue about this point all the time, and I don't have the patience or space on this blog to cite the references, but research tells us that most addicted people need at least three months in treatment to really reduce or stop their drug use and that longer treatment times result in better outcomes. The best programs will measure progress and suggest plans for maintaining recovery. Recovery from drug addiction is a long-term process that often requires several episodes of treatment and ongoing support from family or community. If you have read this far and are starving for the references, contact me.
Relapse does not mean treatment failure. The chronic nature of addiction means that relapsing to drug abuse is not only possible, but likely, similar to what happens with other chronic medical illnesses—such as diabetes, hypertension, and asthma—that have both physical and behavioral components. And like these illnesses, addiction also requires continual evaluation and treatment modification if necessary. A relapse to drug use indicates a need to re-instate or adjust treatment strategy; it does not mean treatment has failed.
5. How do 12-step or similar recovery programs fit into drug addiction treatment?
Self-help groups can complement and extend the effects of professional treatment. The most well-known programs are Alcoholics Anonymous (AA), Narcotics Anonymous (NA), and Cocaine Anonymous (CA), all of which are based on the 12-step model. This group therapy model draws on the social support offered by peer discussion to help promote and sustain drug-free lifestyles.
Most drug addiction treatment programs encourage patients to participate in supportive therapy during and after formal treatment. These groups offer an added layer of community-level social support to help people in recovery with abstinence and other healthy lifestyle goals.
To order NIDA materials, please go to: http://drugpubs.drugabuse.gov.
Science on Will and Willpower - Part II
An excellent video of one of Roy's lectures is on my media page.
We try to control ourselves in all sorts of ways: eating right, exercising, avoiding drugs and alcohol, studying more, working harder, spending less. Baumeister says that the practical significance of all this is enormous. He says: "Most of the problems that plague modern individuals in our society — addiction, overeating, crime, domestic violence, sexually transmitted diseases, prejudice, debt, unwanted pregnancy, educational failure, underperformance at school and work, lack of savings, failure to exercise — have some degree of self control failure as a central aspect."
Baumeister goes on to say that two main traits that seem to produce an immensely broad range of benefits: intelligence and self-control. However, psychology has not found much one can do to produce lasting increases in intelligence. On the other hand, self-control can be strengthened, and the study of self-control is a rare and powerful opportunity for psychology to make a palpable and highly beneficial difference in the lives of ordinary people.
For example, in his research he has found that people perform relatively poorly on tests of self-control when they have engaged in a previous, seemingly unrelated act of self-control: "For instance, in a study in my lab, we invited some students to eat fresh-baked chocolate-chip cookies, and asked others to resist the cookies and munch on radishes instead. Then we gave them impossible geometry puzzles to solve. The students who ate the cookies worked on the puzzles for 20 minutes, on average. But the students who had resisted the tempting cookies gave up after an average of eight minutes."
"Such studies suggest," he continues, "that some willpower was used up by the first task, leaving less for the second. The pattern is opposite to what one would expect based on priming or activating a response mode. So we began to think that some kind of limited resource is at work: It gets depleted as people perform various acts of self-control. Over time, we have begun to link this resource to the folk notion of willpower."
Making decisions seems to use up our willpower. After making decisions, people perform worse at self-control. Conversely, after exerting self-control, decision-making shifts toward simpler and easier processes. That can lead people to make poorer decisions, or to avoid making choices at all. Apparently, decision making depletes the same resource as self-control.
One of Baumeister's examples of willpower depletion: "A dieter may easily avoid a doughnut for breakfast, but after a long day of making difficult decisions at work, he has a much harder time resisting that piece of cake for dessert. Another example might be losing your temper. Normally, you refrain from responding negatively to unpleasant things your romantic partner says. But if one day you’re especially depleted — maybe you’re trying to meet a stressful work deadline — and the person says precisely the wrong thing, you erupt and say the words you would have stifled if your self-control strength was at full capacity. What do you call this process? My collaborators and I use the term “ego depletion” to refer to the state of depleted willpower. Initially, we called it “regulatory depletion” because the first findings focused purely on acts of self-regulation. When it emerged that the same resource was also used for decision-making, we wanted a broader term that would suggest some core aspect of the self was depleted. We borrowed the term “ego” from Freudian theory because Freud had spoken about the self as being partly composed of energy and of processes involving energy."
In his book, Baumeister explains that some people imagine that self-control or willpower is something you only use once in a while, such as when you are tempted to do something wrong. The opposite is true. Research indicates that the average person spends three to four hours a day resisting desires. Self-control is used for other things as well: controlling thoughts and emotions, regulating task performance and making decisions. Most people use their willpower many times a day, all day. And toward the end of the day, there is less gas in the tank.
We now know that people can improve their self-control even as adults. As with a muscle, it gets stronger from regular exercise. So engaging in some extra self-control activities for a couple weeks produces improvement in self-control, even on tasks that have no relation to the exercise activities. The exercises can be arbitrary, such as using your left hand instead of your right hand to open doors and brush your teeth. Or they can be meaningful, such as working to manage money better and save more. The important thing is to practice overriding habitual ways of doing things and exerting deliberate control over your actions. Over time, that practice improves self-control. As people deplete willpower, they became increasingly likely to give in to desires they might otherwise have resisted. This was true for all manner of desires: desires to sleep, to eat, to have sex, to play games, to spend money, to drink alcohol or smoke cigarettes.
One of the best features of Roy Baumeister's work, particularly his book on willpower, is that he is easy to read, accessible to those of us not trained in clinical research or adept at deciphering scientific papers.
Addictionary: Language of Addiction
For example, when the word "alcohol" was written or spoken in early 19th-century America. it was often used in the chemical and medical sense. This is from an article about drawing out the essence of stramonium, or jimson weed: "The virtues of stramonium," the New England Journal of Medicine reported in January of 1818, "appear to be seated in an extractive principle, which dissolves in water and alcohol."
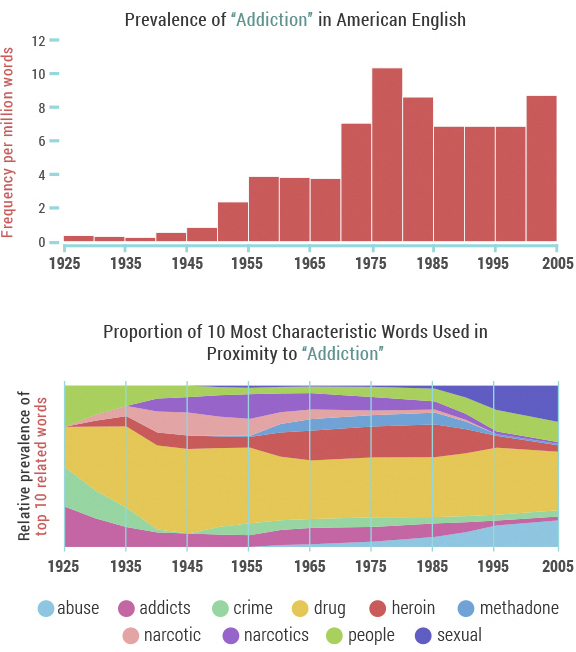
The word "cocaine" had different connotations as well. In the 1860s, for instance, a substance termed "cocaine" was advertised by a Boston company as a topical treatment to prevent hair loss.
Over time these words – "alcohol", "cocaine" and others, including "drugs" and" intoxicated" – became more closely associated with substance use, abuse and addiction in American popular culture.
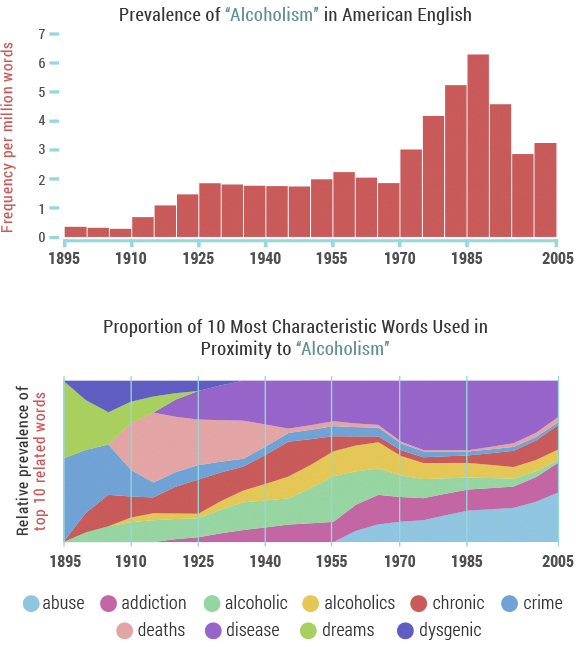
"'Alcoholism' made its debut in the lexicon around 1900, associated almost exclusively with 'crime' and 'dreams' – coincidentally around the time that Sigmund Freud's The Interpretation of Dreams was published," Recovery.org notes. "However, the association with crime was soon eclipsed by concern over 'chronic' alcoholism and 'death'/'deaths' related to alcoholism, which ballooned in the 1920s during the height of the prohibition movement." Documentarian Ken Burns echoes this in his series, Prohibition. One of the tragic unintended consequences of the nationwide crackdown on alcohol was an increase in dangerous, unregulated spirits — leading to 1,000 deaths a year.
Mindfulness Based Relapse Prevention
Traditional treatment for substance abuse often focuses on avoiding or controlling triggers that result in negative emotion or craving. While research has shown that this approach can help, substance abuse relapse remains a problem: about half of those who seek treatment are using again within a year.
Bowen has spent much of her career studying another approach: mindfulness, which involves cultivating moment-to-moment, nonjudgmental awareness of thoughts, feelings, and surroundings. She and her colleagues have developed a program called Mindfulness-Based Relapse Prevention (MBRP), which combines practices like sitting meditation with standard relapse prevention skills, such as identifying events that trigger relapse. Rather than fighting or avoiding the difficult states of mind that arise when withdrawing from a substance, this combination tries to help participants to name and tolerate craving and negative emotion.
But how do mindfulness-based approaches compare to traditional substance abuse treatments? And do mindfulness-based treatments work for everyone? Researchers like Bowen are beginning to answer these questions.
Here is the key to the success of the program: MBRP helps people to relate differently to their thoughts, and use tools to disengage from automatic, addictive behaviors.
The JAMA Psychiatry article describes how effective the Mindfulness-Based Relapse Prevention program is in comparison to a standard relapse-prevention program as well as a conventional 12-step program. Six months following the intervention, the mindfulness-based program and the standard relapse-prevention program were both more successful at reducing relapse than the 12-step program. One year later, the mindfulness-based program proved better than the other two in reducing drinking and drug use.
Bowen says that when people cultivate mindfulness, they’re developing a tool to become aware of that inclination to want only pleasurable things and escape uncomfortable things. Mindfulness also helps people learn to relate to discomfort differently. When an uncomfortable feeling like a craving or anxiety arises, people like Sophia are able to recognize their discomfort, and observe it with presence and compassion, instead of automatically reaching for a drug to make it go away. Bowen says that awareness of our experience and the ability to relate to our experience with compassion gives us more freedom to choose how we respond to discomfort, rather than defaulting to automatic behaviors.
More research is needed to determine why MBRP might be more successful than other programs in reducing substance abuse relapse, but Bowen speculates that MBRP holds an advantage because mindfulness is a tool that can be applied to all aspects of one’s life.
Standard relapse-prevention programs teach tools specific to struggles with substance abuse—for instance, how to deal with cravings or how to say no when someone offers you drugs. A year after completing the program, a person may have a very different set of challenges that the relapse-prevention program did not equip them to deal with.
But because mindfulness is a tool that can be used in every part of a person’s life, practicing moment-to-moment awareness could continue to be an effective coping tool.
James Davis and his colleagues at Duke University are investigating mindfulness training as a way to help people quit smoking. Davis speculates that mindfulness is likely an effective tool in helping people with addiction because it’s a single, simple skill that a person can practice multiple times throughout their day, every day, regardless of the life challenges that arise. With so much opportunity for practice—rather than, say, only practicing when someone offers them a cigarette—people can learn that skill deeply.
Their intervention results showed a significant difference in smoking cessation for people who completed the intervention, as compared to people who were given nicotine patches and counseling from the Tobacco Quit Line.
Both Bowen and Davis emphasize that mindfulness is not a panacea; it doesn’t always work for everyone.
Dr. Zev Schuman-Olivier and his colleagues at the Massachusetts General Hospital Center for Addiction Medicine suggest that the type of therapy a person responds to may have something to do with their disposition. People who had the tendency to treat thoughts and behaviors with non-judgment and acceptance before the intervention began were more likely to be successful in reducing smoking following the mindfulness training. They write that if a person already has the skill to treat the self with non-judgment and acceptance, learning mindfulness practices likely comes easier to them than someone who has not previously practiced this skill.
Ultimately, the type of therapy that works best for a given person will likely capitalize on their pre-disposed strengths.Of course, as Bowen and Davis both note, the skills of mindfulness can be taught to everyone. But Schuman-Olivier’s finding suggests that people who are not oriented toward mindfulness may need a more vigorous or lengthy intervention, in order to more thoroughly learn mindfulness skills. It may be the case that people with less disposition toward mindfulness would fare better with a different therapy.
Another predictor of success in mindfulness-based treatment could be a person’s motivation to engage in the therapy. In Davis’ study, the people that started the intervention with the highest level of nicotine addiction were the most successful in reducing smoking by the end of the treatment. Davis said that this seemingly counterintuitive result likely reflects their motivation to quit; the people that were the most addicted had, at that point, tried everything, and were willing to try their hardest to make this therapy work. Meanwhile, people that were less addicted saw their addiction as less of a problem. They reasoned, “If this doesn’t work, I’ll be ok—something else will work, eventually.” As a result, they were likely less motivated to quit, and less engaged in the therapy.
What Is a Disease?
The ancient Greek academies had differing views of disease. Hippocrates emphasized the sick individual with his particular kind of misery. Others saw disease as a specific pathological process, evidenced by a visible sign such as a tumor, wound, or physical symptom. To this day, the definition of disease remains controversial. The AMA Council on Science and Public Health recently addressed the question, “Is obesity a disease?” The Council’s response: “Without a single, clear, authoritative, and widely accepted definition of disease, it is difficult to determine conclusively whether or not obesity is a medical disease state.”
This is also true for the vast majority of psychiatric disorders, particularly the addictions. The individual’s degree of suffering and incapacity—or distress and dysfunction—defines a state of disease. Although we now have some clues about the causes of mental disorders, and neuroimaging studies are making great strides, the American Psychiatric Association takes this position:
“The exact causes of mental disorders are unknown, but an explosive growth of research has brought us closer to the answers. We can say that certain inherited dispositions interact with triggering environmental factors. Poverty and stress are well-known to be bad for your health—this is true for mental health and physical health. In fact, the distinction between “mental” illness and “physical” illness can be misleading. Like physical illnesses, mental disorders can have a biological nature. Many physical illnesses can also have a strong emotional component.”
The National Alliance on Mental Illness (NAMI) seems to agree: “A mental illness is a condition that impacts a person's thinking, feeling or mood may affect and his or her ability to relate to others and function on a daily basis. Each person will have different experiences, even people with the same diagnosis. Recovery, including meaningful roles in social life, school and work, is possible, especially when you start treatment early and play a strong role in your own recovery process. A mental health condition isn’t the result of one event. Research suggests multiple, interlinking causes. Genetics, environment and lifestyle combine to influence whether someone develops a mental health condition. A stressful job or home life makes some people more susceptible, as do traumatic life events like being the victim of a crime. Biochemical processes and circuits as well as basic brain structure may play a role too.”
These questions highlight the importance of seeing the suffering person as more than a diagnosis or a label. This is the message I emphasize in my presentation, “Four Sides to Every Story,” available on request. Diagnosis is helpful, because we know that certain treatments are effective for certain diseases. For example, some fevers are caused by infection, and if we kill the offending bug we can cure the disease. Other fevers are caused by inflammation—as in rheumatoid arthritis or drug reactions—and if we calm the inflammation we can ease the fever.
At the same time, the psychiatrist should see much more than a label or a diagnosis (what the patient has in terms of the disease model). The psychiatrist—or any mental health professional—should also take the other three perspectives into account: who the person is, what the person does, and what the person has encountered. Using all four perspectives, the disease model can be valuable. It’s just not the whole story.
Painkillers, Narcotic Abuse, and Addiction
Over the past twenty years, drugs like hydrocodone, oxycontin, and similar narcotics have become an epidemic problem.
Opioids -- also called opiates or narcotics -- are pain relievers made from opium, which comes from the poppy plant. Morphine and codeine are the two natural products of opium. Synthetic modifications or imitations of morphine produce the other opioids:
Heroin (street drug)
Dilaudid (hydromorphone)
Percocet, Percodan, OxyContin (oxycodone)
Vicodin, Lorcet, Lortab (hydrocodone)
Demerol (pethidine)
Methadone
Duragesic (fentanyl)
When people use narcotics only to control pain, they are unlikely to become addicted to the drugs. However, opioids provide an intoxicating high when injected or taken orally in high doses. Opioids are also powerful anxiety relievers. For these reasons, narcotic abuse is one of the most common forms of drug abuse in the U.S.
Terms like opioid abuse, drug abuse, drug dependence, and drug addiction are often used interchangeably, but experts define them as follows:
Drug abuse, including opioid abuse, is the deliberate use of a medicine beyond a doctor's prescription. In the case of opiates, the intention is generally to get high or to relieve anxiety.
Dependence occurs when the body develops tolerance to the drug, meaning higher doses are needed for the same effect. In addition, stopping the drug produces drug withdrawal symptoms.
Drug addiction occurs when the person has drug dependence, but also displays psychological effects. These include compulsive behavior to get the drug; craving for the drug; and continued use despite negative consequences, like legal problems or losing a job.
Symptoms of Narcotic Abuse
Signs and symptoms of opioid abuse include:
- Analgesia (feeling no pain)
- Sedation
- Euphoria (feeling high)
- Respiratory depression (shallow or slow breathing)
- Small pupils
- Nausea, vomiting
- Itching or flushed skin
- Constipation
- Slurred speech
- Confusion or poor judgment
Symptoms of Opioid Drug Withdrawal
If a person uses opioids for a long time, they develop physical dependence and tolerance. Usually, opioid abusers will then take more of the drug, to continue to get high. If a person stops using opioids after they become physically dependent on the drug, they will experience drug withdrawal symptoms which can include:
Anxiety
Irritability
Craving for the drug
Rapid breathing
Yawning
Runny nose
Salivation
Gooseflesh
Nasal stuffiness
Muscle aches
Vomiting
Abdominal cramping
Diarrhea
Sweating
Confusion
Enlarged pupils
Tremors
Loss of appetite
I tell patients that withdrawal from drugs like painkillers and heroin is like the worst case of the flu you've ever experienced. The symptoms of opioid drug withdrawal can be agonizing and intolerable, contributing to continued drug abuse. In general, how severe opioid drug withdrawal symptoms are, and how long they last, depends on how long the person has been abusing opioids and how much they have been taking.
Medicines like methadone, buprenorphine (sometimes combined with naloxone), and naltrexone can be taken in various forms and are used to prevent withdrawal symptoms after a person stops using, a process called detoxification ("detox"). After drug withdrawal is complete, the person is no longer physically dependent on the drug. But psychological dependence can continue. Some people with drug addiction may relapse in response to stress or other powerful triggers.
Dependence vs. Addiction
Controlling pain is the goal when opioids are used medically. Patients or health care professionals should not let fear of addiction prevent them from using opioids for effective pain relief. Knowing the difference between dependence and addiction is important.
People who take opioids for pain relief for extended periods of time may need higher doses to ease their pain. They may develop tolerance to the drug and experience withdrawal symptoms if the medication is abruptly stopped. They become physically dependent on the drug.
Addiction occurs when narcotic abuse becomes compulsive and self-destructive, especially concerning an opioid user's need to use the drug for reasons other than pain relief.
To prevent withdrawal symptoms in people who have become physically dependent on opioids for pain relief, the dose may be slowly lowered over a few weeks. People who are weaned off opioids and are pain free usually don't start taking the drug again or become abusers of narcotics. Opioids used for short-term medical conditions rarely require weaning. In those cases, stopping the medication after a brief period usually doesn't cause withdrawal symptoms.
Other Abused Drugs
Strictly speaking, most drugs referred to informally as narcotics really aren't. However, two drug classes have some similar effects to opioids, when abused:
Benzodiazepines include Valium, Ativan, and Xanax. Benzodiazepine abuse results in sedation and calm, but tolerance develops rapidly. Withdrawal can result in seizures, unlike opioid withdrawal.
Barbiturates include Seconal, Amytal, Nembutal, and Luminal. Barbiturates are also sedating and calming. Withdrawal after continued barbiturate abuse, like benzodiazepine abuse, is medically serious.
In general, benzodiazepines and barbiturates have less pain-relieving effects than opioids. All three drug classes are sedating and anxiety-relieving. Benzodiazepine abuse, barbiturate abuse, and narcotic abuse all produce tolerance and physical dependence over time, and withdrawal symptoms after sudden discontinuation.
This post includes material from WebMD Medical Reference.
SOURCES:
Van den Brink, W. Canadian Journal of Psychiatry, 2006.
WebMD Medical Reference: "Narcotic Abuse."
Bateson, A.N. Current Pharmaceutical Design, January 2002.
eMedicine.com: "Toxicity, Barbiturate."
Reviewed by Arefa Cassoobhoy, MD, MPH on August 01, 2013
Do 12-Step Programs Work?
Since the 1930's when Bill W. and Dr. Bob started Alcoholics Anonymous (AA) the fellowship has grown to over two million members. Meeting in rented rooms, school halls, hospitals, and the storied church basement, AA and similar 12-step organizations (eg, Narcotics Anonymous [NA]) remain the most commonly sought sources of help for substance-related problems in the United States (Substance Abuse and Mental Health Services Administration. Results from the 2007 National Survey on Drug Use and Health: National Findings. Rockville, MD: Office of Applied Studies; 2008).
Research has shown that attending AA, either alone or during and following professional treatment, enhances outcomes. One naturalistic study, for example, followed 466 previously untreated individuals with problem drinking for eight years. Participants self-selected into one of four groups: no treatment, AA alone, formal treatment alone, and formal treatment plus AA. Those who received some sort of help—AA, formal treatment, or both—had higher rates of abstinence at all time points. At eight years, 26% of patients in the no treatment group were abstinent from alcohol compared to 49% who received AA alone, 46% who received formal treatment alone, and 58% who received the combination of treatment plus AA (Timko C et al, J Stud Alcohol 2000;61(4):529–540).
A systematic Cochrane review of the best scientific studies on AA and TSF found that they were as effective as any of the interventions to which they were compared for some factors, such as retention in treatment, but found that no studies unequivocally proved AA and TSF were superior to other treatments (Ferri M et al, Cochrane Database Syst Rev 2006;(3):CD005032).
Other studies have found a linear dose-response relationship between AA attendance and favorable drinking outcomes (Kaskutas LA, J Addict Dis 2009;28(2):145–157). Attending one meeting per week, on average, appears to be the minimum threshold to realize benefit and increasing meeting frequency is associated with progressively greater rates of abstinence. In addition, research has shown that women engage with AA as much as men, become more involved with the 12 Steps, and derive similar benefit. In 1990, the Institute of Medicine called for more research on how AA works. Since then, research has revealed that AA aids recovery through multiple mechanisms, many of which are also activated by professional behavioral treatments (Kelly J et al, Addict Res Theory 2009:17(3):236–259).
Most consistently and strongly, AA appears to work by helping people make positive changes in their social networks (eg, by dropping heavy drinkers/drug users and increasing abstainers/low risk drinkers), and by enhancing coping skills and self-efficacy for abstinence when encountering high-risk social situations (see for example, Kelly JF et al, Drug Alcohol Depend 2011;114(2–3):119–126).
Among more severely addicted people, AA also appears to work by enhancing spiritual practices, reducing depression, and increasing individuals’ confidence in their ability to cope with negative emotion (Kelly JF et al, Addiction 2012;107(2)289–299). Thus, AA appears to work through diverse mechanisms and may work differently for different people. Stated another way: individuals may use AA differently, depending on their unique needs and challenges.
Research has shown that involvement in 12-step work can reduce the need for more costly treatments while simultaneously improving outcomes. A large multicenter study of over 1,700 patients found those treated in professional 12-step treatment went on to participate in community-based AA and NA meetings at a higher rate than those from professional cognitive behavioral therapy (CBT) programs, who relied more heavily on professional services. This translated into a two-year savings of over $8,000 per patient among 12-step treated patients, without compromising outcomes. In fact, those treated in the 12-step treatment programs had one-third higher rates of abstinence across follow-up (Humphreys K & Moos R, Clin Exp Res 2001;25(5):711–716; Humphreys & Moos, Alcohol Clin Exp Res 2007;31(1):64–68).
Project MATCH was a large randomized trial comparing three individually-delivered psychosocial treatments for alcohol use disorder—TSF, CBT, and Motivational Enhancement Therapy (MET)—that was funded by NIAAA. It included 1,726 patients from nine clinical sites across the US (Project Match Research Group, J Stud Alcohol 1997;58(1):7–29). TSF was found to be as effective as the more empirically supported CBT and MET interventions at reducing the quantity and frequency of alcohol use post-treatment and at one- and three-year follow-ups. Moreover, TSF was superior to CBT and MET at increasing rates of continuous abstinence, such that 24 percent of the outpatients in the TSF condition were continuously abstinent at one year after treatment, compared with 15 percent and 14 percent in CBT and MET, respectively (Tonigan JS et al,Participation and involvement in Alcoholics Anonymous. In: Babor TF & Del Boca FK, eds. Treatment Matching in Alcoholism. New York: Cambridge University Press;2003:184–204).
Abstinence rates at three years continued to favor TSF, with 36 percet reporting complete abstinence, compared with 24 percent in CBT, and 27 percent in MET (Cooney N et al. Clinical and scientific implications of Project MATCH. In: Babor TF & Del Boca FK, eds. Treatment Matching in Alcoholism. New York: Cambridge University Press; 2003:222–237).
In light of findings from several such RCTs that demonstrated the efficacy of TSF, this therapy was added to the Substance Abuse and Mental Health Services Administration’s (SAMHSA) National Registry of Evidence-Based Practices and Programs (NREPP) in 2008.
The overwhelming majority of research has been conducted on AA. More research is needed on other MHOs, such as SMART Recovery, LifeRing, Celebrate Recovery, Women for Sobriety, Moderation Management, and others, so that more objective evidence is gathered on secular, religious, and non-abstinence-based AA alternatives (see the article "Alternatives to 12-Step Recovery" for more on these groups).
Two Talks Today to Good Teams
Thoughts and Reflections
Psychiatry as a medical specialty is a vast—and often uncharted—territory. The basic education of a psychiatrist is highly scientific and technical. The first two years of medical school are purely basic science: anatomy, physiology, biochemistry, microbiology, and so on. The last two years include brief exposure to psychiatry and psychology, but most of the time is devoted to medicine, surgery, ob-gyn, and pediatrics. Internship and residency years in psychiatry involve patient care, but the psychiatrist’s true education begins after graduation. As the venerable Dr. Eugene Stead used to tell us at Duke, “Medical school is where you stay until you’re old enough to learn how to be a doctor.” The education of the good psychiatrist is a process that lasts a lifetime.
Thanks for reading!