June 2015
Bogus: Dr. Oz
Medical students and residents frustrated with bogus advice from doctors on TV have, for more than a year, been asking the American Medical Association to clamp down and "defend the integrity of the profession."
This is an issue I have addressed before on this blog where my focus has been on quackery associated with the use of expensive neuroimaging or "brain scans" claiming to diagnose a variety of psychiatric problems like attention deficit disorder, addictions, and mood problems. Although neuroimaging is very promising, getting a scan does not change diagnosis or treatment for these kinds of disorders. One of the egregious offenders is Dr. Daniel Amen, perhaps the best known psychiatrist in America, whose self-produced PBS specials air widely on public television and promote his unproven claims about scans. Although Amen claims that his theories are based on thousands of cases, experts in the field have widely condemned his misrepresentation of the facts.
The AMA is finally taking a stand on quack doctors who spread pseudoscience in the media.
The AMA will look at creating ethical guidelines for physicians in the media, write a report on how doctors may be disciplined for violating medical ethics through their press involvement, and release a public statement denouncing the dissemination of dubious medical information through the radio, TV, newspapers, or websites.The move came out of the AMA's annual meeting in Chicago this week, where medical students and residents pushed the AMA after noticing that the organization was mostly silent during the recent public debates about the ethics of Dr. Oz sharing unfounded medical advice on his exceptionally popular TV show.
"Dr. Oz has something like 4 million viewers a day," student representatives said. "The average physician doesn't see a million patients in their lifetime. That's why organized medicine should be taking action."
Last summer, Oz was called before a Senate subcommittee on consumer protection, where the senator in charge, Claire McCaskill (D-MO), asked him to explain his use of "flowery" language to champion weight loss fixes that don't actually work and then admonished him for endorsing a rainbow of supplements as potential "belly blasters"and "mega metabolism boosters." As McCaskill put it, "The scientific community is almost monolithic against you in terms of the efficacy of the three products you called 'miracles.'"
In December, a British Medical Journal study examined the health claims showcased on 40 randomly selected episodes of the two most popular internationally syndicated health talk shows — The Dr. Oz Show and The Doctors — and found that about half of the recommendations either had no evidence behind them or actually contradicted the best available science.
In January, investigations into The Dr. Oz Show by the Federal Trade Commission showed that at least one of Oz's miracle-touting guests used the program as a platform to deceive audiences and sell products.
In April, a high-profile group of physicians and academics questioned Oz's faculty position at Columbia University and wrote in a letter to the medical school dean: "Dr. Oz is guilty of either outrageous conflicts of interest or flawed judgments about what constitutes appropriate medical treatments, or both." The same month, Oz responded to his critics by accusing them of having conflicts of interest and defending his civil liberties. "I know I have irritated some potential allies," he wrote in Time magazine. "No matter our disagreements, freedom of speech is the most fundamental right we have as Americans. We will not be silenced."
What Dr. Oz does not understand is that questions about ethics are not questions about "free speech." By his logic, a doctor can say virtually anything, make any claim, asserting that he or she has the right to freedom of speech. This is a terrible kind of logic, and it makes no sense at all.
Then again, many claims made by Dr. Oz make no sense, either.
This is an issue I have addressed before on this blog where my focus has been on quackery associated with the use of expensive neuroimaging or "brain scans" claiming to diagnose a variety of psychiatric problems like attention deficit disorder, addictions, and mood problems. Although neuroimaging is very promising, getting a scan does not change diagnosis or treatment for these kinds of disorders. One of the egregious offenders is Dr. Daniel Amen, perhaps the best known psychiatrist in America, whose self-produced PBS specials air widely on public television and promote his unproven claims about scans. Although Amen claims that his theories are based on thousands of cases, experts in the field have widely condemned his misrepresentation of the facts.
The AMA is finally taking a stand on quack doctors who spread pseudoscience in the media.
The AMA will look at creating ethical guidelines for physicians in the media, write a report on how doctors may be disciplined for violating medical ethics through their press involvement, and release a public statement denouncing the dissemination of dubious medical information through the radio, TV, newspapers, or websites.The move came out of the AMA's annual meeting in Chicago this week, where medical students and residents pushed the AMA after noticing that the organization was mostly silent during the recent public debates about the ethics of Dr. Oz sharing unfounded medical advice on his exceptionally popular TV show.
"Dr. Oz has something like 4 million viewers a day," student representatives said. "The average physician doesn't see a million patients in their lifetime. That's why organized medicine should be taking action."
Last summer, Oz was called before a Senate subcommittee on consumer protection, where the senator in charge, Claire McCaskill (D-MO), asked him to explain his use of "flowery" language to champion weight loss fixes that don't actually work and then admonished him for endorsing a rainbow of supplements as potential "belly blasters"and "mega metabolism boosters." As McCaskill put it, "The scientific community is almost monolithic against you in terms of the efficacy of the three products you called 'miracles.'"
In December, a British Medical Journal study examined the health claims showcased on 40 randomly selected episodes of the two most popular internationally syndicated health talk shows — The Dr. Oz Show and The Doctors — and found that about half of the recommendations either had no evidence behind them or actually contradicted the best available science.
In January, investigations into The Dr. Oz Show by the Federal Trade Commission showed that at least one of Oz's miracle-touting guests used the program as a platform to deceive audiences and sell products.
In April, a high-profile group of physicians and academics questioned Oz's faculty position at Columbia University and wrote in a letter to the medical school dean: "Dr. Oz is guilty of either outrageous conflicts of interest or flawed judgments about what constitutes appropriate medical treatments, or both." The same month, Oz responded to his critics by accusing them of having conflicts of interest and defending his civil liberties. "I know I have irritated some potential allies," he wrote in Time magazine. "No matter our disagreements, freedom of speech is the most fundamental right we have as Americans. We will not be silenced."
What Dr. Oz does not understand is that questions about ethics are not questions about "free speech." By his logic, a doctor can say virtually anything, make any claim, asserting that he or she has the right to freedom of speech. This is a terrible kind of logic, and it makes no sense at all.
Then again, many claims made by Dr. Oz make no sense, either.
One Nation, Under Sedation
06/11/15 18:55 Filed in: Psychiatry | Addiction Medicine
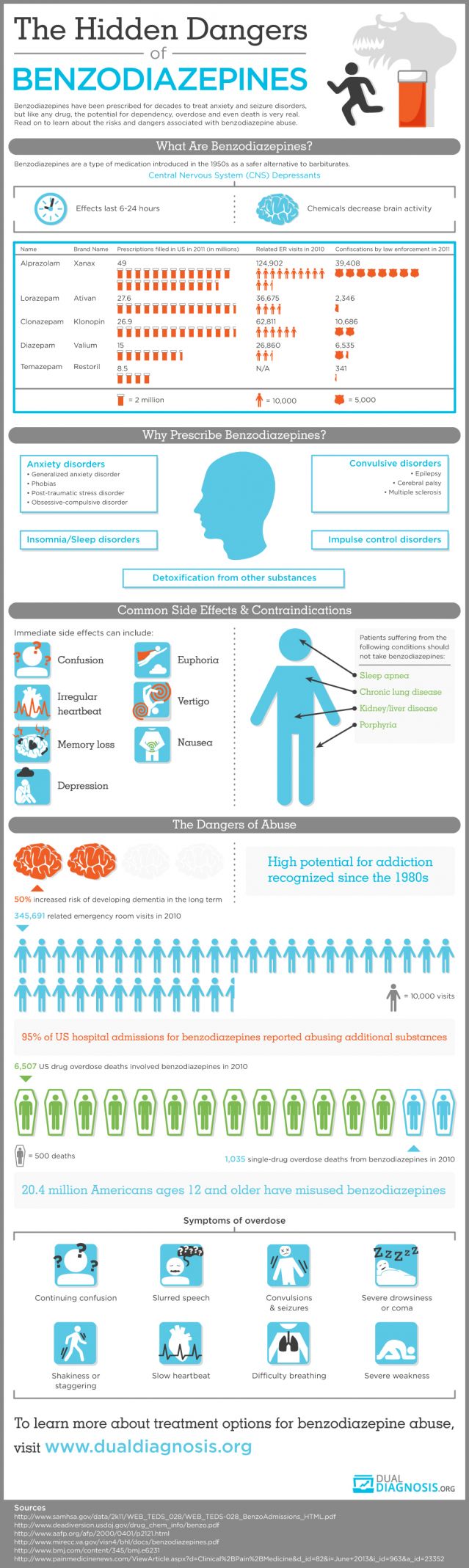
In 2012, Medicare’s massive prescription drug program didn’t spend a penny on popular tranquilizers such as Valium, Xanax and Ativan. The following year, it doled out more than $377 million for the drugs.
Houston, we have a problem. For the full story, click here.
The distinguished addiction specialist Charles O'Brien, M.D., authored a paper in 2005 discussing the risks of benzodiazepine abuse. The summary of his article states: "Although benzodiazepines are invaluable in the treatment of anxiety disorders, they have some potential for abuse and may cause dependence or addiction. It is important to distinguish between addiction to and normal physical dependence on benzodiazepines. Intentional abusers of benzodiazepines usually have other substance abuse problems. Benzodiazepines are usually a secondary drug of abuse-used mainly to augment the high received from another drug or to offset the adverse effects of other drugs. Few cases of addiction arise from legitimate use of benzodiazepines. Pharmacologic dependence, a predictable and natural adaptation of a body system long accustomed to the presence of a drug, may occur in patients taking therapeutic doses of benzodiazepines. However, this dependence, which generally manifests itself in withdrawal symptoms upon the abrupt discontinuation of the medication, may be controlled and ended through dose tapering, medication switching, and/or medication augmentation. Due to the chronic nature of anxiety, long-term low-dose benzodiazepine treatment may be necessary for some patients; this continuation of treatment should not be considered abuse or addiction."
Houston, we have a problem. For the full story, click here.
The distinguished addiction specialist Charles O'Brien, M.D., authored a paper in 2005 discussing the risks of benzodiazepine abuse. The summary of his article states: "Although benzodiazepines are invaluable in the treatment of anxiety disorders, they have some potential for abuse and may cause dependence or addiction. It is important to distinguish between addiction to and normal physical dependence on benzodiazepines. Intentional abusers of benzodiazepines usually have other substance abuse problems. Benzodiazepines are usually a secondary drug of abuse-used mainly to augment the high received from another drug or to offset the adverse effects of other drugs. Few cases of addiction arise from legitimate use of benzodiazepines. Pharmacologic dependence, a predictable and natural adaptation of a body system long accustomed to the presence of a drug, may occur in patients taking therapeutic doses of benzodiazepines. However, this dependence, which generally manifests itself in withdrawal symptoms upon the abrupt discontinuation of the medication, may be controlled and ended through dose tapering, medication switching, and/or medication augmentation. Due to the chronic nature of anxiety, long-term low-dose benzodiazepine treatment may be necessary for some patients; this continuation of treatment should not be considered abuse or addiction."
Female Veteran Suicides
My first experience working with our veterans was during the Vietnam era, when I trained at Duke University Medical Center and The University of Wisconsin Medical Center. Fifteen years ago I was the first director of our UT Southwestern Addiction Psychiatry Fellowship Program, and our primary clinical service was at The North Texas VA Healthcare System ("the VA Hospital") in Dallas. Compared to the 1970's, the military today is increasingly diverse, and for the first time we are treating many women who have served in our armed forces. The latest studies on suicide in the military are alarming. The 2012 VA Report on Suicide can be found here, and the main findings are cited below.
Women are generally a lot less likely to kill themselves than men, but female veterans are an exception with shockingly high suicide rates, according to new Veterans Affairs Department research. Among women of all ages who have served in the military, the suicide rate is 28.7 per 100,000—higher than the rate among male civilians, nearly six times the rate of civilian women, and approaching the 32.1 rate among male veterans. "It's staggering," a Northeastern University epidemiologist said to the Los Angeles Times. "We have to come to grips with why the rates are so obscenely high." Women vets ages 18 to 29 kill themselves at nearly 12 times the rate of civilian women the same age, but the rate was up to eight times higher even among women who served in the 1950s. It is not clear what is driving the rates. VA researchers and experts who reviewed the data for The Times said there were myriad possibilities, including whether the military had disproportionately drawn women at higher suicide risk and whether sexual assault and other traumatic experiences while serving played a role.
The VA suicide study involved data on 173,969 adult suicides in 23 states over 11 years, which included the deaths of 40,571 male vets and 2,637 female vets. The article in Psychiatric Services also says that that people who join the military are more likely to have had troubled childhoods; and it could be the case that women who signed up were at higher risk of suicide in the first place.
• While the percentage of all suicides reported as Veterans has decreased, the number of suicides has increased.
• A majority of Veteran suicides are among those age 50 years and older.
• Male Veterans who die by suicide are older than non-Veteran males who die by suicide.
• The age distribution of Veteran and non-Veteran women who have died from suicide is similar.
• The demographic characteristics of Veterans who have died from suicide are similar among those with and without a history of VHA service use.
• Among those at risk, the first 4 weeks following service require intensive monitoring and case management. • There is preliminary evidence in 2012 indicating a decrease in the rate of non-fatal suicide events for VHA utilizing Veterans.
• Decreasing rates of non-fatal suicide events are associated with increasing age.
• The data show a decrease in the 12 month re-event prevalence in fiscal year (FY) 2012.
• The majority of Veterans who have a suicide event were last seen in an outpatient setting.
• A high prevalence of non-fatal suicide events result from overdose or other intentional poisoning.
• Continued increases in calls to the Veterans Crisis Line may be associated with efforts to enhance awareness of VHA services through public education campaigns.
• The majority of callers to the Veterans Crisis Line are male and between the ages of 50- 59.
• Differences in the age composition of callers to the Veterans Crisis Line are associated with gender.
• A large percentage of callers to the Veterans Crisis Line are identified as Veterans.
• Approximately 19 percent of callers to the Veterans Crisis Line call more than once each month.
• The percentage of callers to the Veterans Crisis Line who are currently thinking of suicide has decreased.
• The percentage of all calls resulting in a rescue has decreased, indicating that the calls are less emergent and callers are using the Crisis Line earlier.
• The percentage of callers receiving a referral for follow-up care is increasing.
• Approximately 93 percent of all Veterans Crisis Line referrals are made to callers with a history of VHA service use in the past 12 months.
• Service use continues to increase following a referral for care.
• Between FY 2009 – FY 2011, use of inpatient and outpatient services increased following a rescue.
• The 12 month re-event prevalence has decreased among those who have been rescued or received a referral for follow-up care.
Women are generally a lot less likely to kill themselves than men, but female veterans are an exception with shockingly high suicide rates, according to new Veterans Affairs Department research. Among women of all ages who have served in the military, the suicide rate is 28.7 per 100,000—higher than the rate among male civilians, nearly six times the rate of civilian women, and approaching the 32.1 rate among male veterans. "It's staggering," a Northeastern University epidemiologist said to the Los Angeles Times. "We have to come to grips with why the rates are so obscenely high." Women vets ages 18 to 29 kill themselves at nearly 12 times the rate of civilian women the same age, but the rate was up to eight times higher even among women who served in the 1950s. It is not clear what is driving the rates. VA researchers and experts who reviewed the data for The Times said there were myriad possibilities, including whether the military had disproportionately drawn women at higher suicide risk and whether sexual assault and other traumatic experiences while serving played a role.
The VA suicide study involved data on 173,969 adult suicides in 23 states over 11 years, which included the deaths of 40,571 male vets and 2,637 female vets. The article in Psychiatric Services also says that that people who join the military are more likely to have had troubled childhoods; and it could be the case that women who signed up were at higher risk of suicide in the first place.
• While the percentage of all suicides reported as Veterans has decreased, the number of suicides has increased.
• A majority of Veteran suicides are among those age 50 years and older.
• Male Veterans who die by suicide are older than non-Veteran males who die by suicide.
• The age distribution of Veteran and non-Veteran women who have died from suicide is similar.
• The demographic characteristics of Veterans who have died from suicide are similar among those with and without a history of VHA service use.
• Among those at risk, the first 4 weeks following service require intensive monitoring and case management. • There is preliminary evidence in 2012 indicating a decrease in the rate of non-fatal suicide events for VHA utilizing Veterans.
• Decreasing rates of non-fatal suicide events are associated with increasing age.
• The data show a decrease in the 12 month re-event prevalence in fiscal year (FY) 2012.
• The majority of Veterans who have a suicide event were last seen in an outpatient setting.
• A high prevalence of non-fatal suicide events result from overdose or other intentional poisoning.
• Continued increases in calls to the Veterans Crisis Line may be associated with efforts to enhance awareness of VHA services through public education campaigns.
• The majority of callers to the Veterans Crisis Line are male and between the ages of 50- 59.
• Differences in the age composition of callers to the Veterans Crisis Line are associated with gender.
• A large percentage of callers to the Veterans Crisis Line are identified as Veterans.
• Approximately 19 percent of callers to the Veterans Crisis Line call more than once each month.
• The percentage of callers to the Veterans Crisis Line who are currently thinking of suicide has decreased.
• The percentage of all calls resulting in a rescue has decreased, indicating that the calls are less emergent and callers are using the Crisis Line earlier.
• The percentage of callers receiving a referral for follow-up care is increasing.
• Approximately 93 percent of all Veterans Crisis Line referrals are made to callers with a history of VHA service use in the past 12 months.
• Service use continues to increase following a referral for care.
• Between FY 2009 – FY 2011, use of inpatient and outpatient services increased following a rescue.
• The 12 month re-event prevalence has decreased among those who have been rescued or received a referral for follow-up care.
New Brain Discovery? Lymph!
06/08/15 17:16 Filed in: Neuroscience | Brain Health
Although we don't know for certain that new treatments are just over the horizon, here's some potentially exciting news. Scientists at the University of Virginia have discovered previously unknown lymphatic vessels in the outer layers of the brain. These vessels appeared to link the brain and spinal cord with the rest of the body’s immune system. This study used mice and human samples, vessel structure was investigated in the mice, and the observations followed up in the human samples. This was an animal study using mice to investigate the structure and function of lymphatic vessels in the brain. In fact, this story has been circulating for awhile, but recently it's been highlighted in several stories. The good news is that this may mean that the original studies are standing up to scrutiny by other scientists.
The discovery may require a reassessment of our assumptions about lymph drainage in the brain and its role in diseases involving brain inflammation or degeneration, such as Alzheimer’s disease and multiple sclerosis. The study was published in the peer-reviewed scientific journal Nature.
When I was in medical school, we were taught that the central nervous system (brain and spinal cord) did not have a typical lymphatic drainage system. Lymph is the immune fluid that circulates through the body, containing white blood cells to fight infection and destroy abnormal cells. This study aimed to look at the circulation of lymph in the mouse brain, but mice and humans do not have identical biology, so the findings may not be directly applicable.
The study involved complex laboratory techniques, using a fluorescent antibody to assess the alignment of cells within the brain, examination for markers associated with a lymphatic drainage system and looking at the functional capacity of identified vessels to carry lymphatic fluid to and from the brain.
Human samples taken from the brain at autopsy were used to investigate any structures found in mice.
The scientists found that the outer protective layers of the mouse brain showed cells that were clearly lined up, which suggested that these were vessels with a unique function. These cells showed the characteristic features of functional lymphatic vessels. These vessels appeared able to carry both fluid and immune cells from the fluid surrounding the brain and spinal cord (the cerebrospinal fluid), and were connected to the lymph nodes in the neck. The location of these vessels may have been the reason they have not been discovered before, thereby causing the belief that there is no lymphatic drainage system in the brain.
This may mean current thinking about how the brain works needs to be reassessed. The researchers go on to say it could be the malfunction of these vessels that could be the cause of a variety of brain disorders, such as multiple sclerosis and Alzheimer’s disease.
Summary: This mouse study has examined the circulation of lymph in the brain. It discovered previously unknown lymphatic vessels in the outer layers of the mouse brain. If accurate, the findings may call for a review of how the immune system in the brain functions, and shed new light on its role in brain diseases involving brain inflammation or degeneration. Though animal research can give a good insight into biological and disease processes, and how they may work in humans, the processes in humans and mice are not identical. Further studies are needed to confirm these findings and to assess whether this knowledge is transferable to humans. As such, it is too early to say whether the findings could one day have any implications for the treatment of degenerative brain conditions such as multiple sclerosis or Alzheimer’s.
The original article in Nature can be found here.
The discovery may require a reassessment of our assumptions about lymph drainage in the brain and its role in diseases involving brain inflammation or degeneration, such as Alzheimer’s disease and multiple sclerosis. The study was published in the peer-reviewed scientific journal Nature.
When I was in medical school, we were taught that the central nervous system (brain and spinal cord) did not have a typical lymphatic drainage system. Lymph is the immune fluid that circulates through the body, containing white blood cells to fight infection and destroy abnormal cells. This study aimed to look at the circulation of lymph in the mouse brain, but mice and humans do not have identical biology, so the findings may not be directly applicable.
The study involved complex laboratory techniques, using a fluorescent antibody to assess the alignment of cells within the brain, examination for markers associated with a lymphatic drainage system and looking at the functional capacity of identified vessels to carry lymphatic fluid to and from the brain.
Human samples taken from the brain at autopsy were used to investigate any structures found in mice.
The scientists found that the outer protective layers of the mouse brain showed cells that were clearly lined up, which suggested that these were vessels with a unique function. These cells showed the characteristic features of functional lymphatic vessels. These vessels appeared able to carry both fluid and immune cells from the fluid surrounding the brain and spinal cord (the cerebrospinal fluid), and were connected to the lymph nodes in the neck. The location of these vessels may have been the reason they have not been discovered before, thereby causing the belief that there is no lymphatic drainage system in the brain.
This may mean current thinking about how the brain works needs to be reassessed. The researchers go on to say it could be the malfunction of these vessels that could be the cause of a variety of brain disorders, such as multiple sclerosis and Alzheimer’s disease.
Summary: This mouse study has examined the circulation of lymph in the brain. It discovered previously unknown lymphatic vessels in the outer layers of the mouse brain. If accurate, the findings may call for a review of how the immune system in the brain functions, and shed new light on its role in brain diseases involving brain inflammation or degeneration. Though animal research can give a good insight into biological and disease processes, and how they may work in humans, the processes in humans and mice are not identical. Further studies are needed to confirm these findings and to assess whether this knowledge is transferable to humans. As such, it is too early to say whether the findings could one day have any implications for the treatment of degenerative brain conditions such as multiple sclerosis or Alzheimer’s.
The original article in Nature can be found here.
Brain Scan Scams: Amen!
06/07/15 16:47 Filed in: Psychiatry
At least once a week I am asked about neuroscience and brain scans, usually by someone baffled by a psychiatric problem. I addressed "brain scams" in a blog post here back in April, and I've found another well-done article from The Washington Post describing the fame and the quackery of Dr. Daniel Amen, known for his self-produced PBS television shows and his many pseudoscientific books. Dr. Amen, who lives in a $4M home in California, is the poster child for what is worst in psychiatry. Although Amen has his admirers, the leaders of American psychiatry are not among his fans. The following paragraphs are excerpted and edited from the Washington Post article. The bottom line is this: There are situations, including some brain injuries, where a brain scan can be helpful in making a diagnosis. Brain scans today, however, cannot diagnose psychiatric disorders; nor do these expensive scans change the course of proper psychiatric care.
What the reader should understand is that Dr. Amen, like many promoters of fraudulent "cures," appeals to people who are vulnerable to snake-oil promotions and great salesmanship. He has even hornswoggled fellow entrepreneurial genius Rick Warren, best known for The Purpose Driven Life, and pastor of the Saddleback Church in California. Warren designated Amen as official guru for health and nutrition at his mega-church.
Few top researchers and scientists say that SPECT is anything but a research tool of limited clinical use in identifying strokes, brain injuries and the like. It is helpful in group studies, to say broad things about groups of patients, but not specific things about individual patients. And, researchers say, SPECT has largely since been surpassed by technologies such as PET and functional MRIs, which give images of far greater clarity. It’s no longer viewed as cutting edge.
The APA first debunked many of Amen’s SPECT claims in a 2005 report. In 2008, Carlat, the Tufts professor and author, went to California to test Amen’s clinic. He then wrote, in Wired Magazine, that the black-clad Amen looked “more like a Miami maitre d’ than a psychiatrist,” that the SPECT scan was “spectacularly meaningless” and that Amen’s analysis of it reminded him of a “shrewd palm reader.”
In 2010, Thomas Insel, director of the NIMH, wrote on his blog that while the technology “might be playing in prime time on some TV infomercials, brain-imaging experts say we’re not quite there yet.” Earlier this year, Anissa Abi-Dargham, a highly regarded professor of clinical psychiatry and radiology at Columbia who has done extensive work with brain imaging, spoke at an APA symposium on the limits of SPECT. She listened to Amen’s hour-long lecture there. Reached by phone recently, she said: “Had I known what this was, I would have never agreed to be part of it. It was not a scientific debate. It was propaganda for his clinics.”
No major research institution takes his SPECT work seriously, none regards him as “the number one neuroscience guy,” and his revelations, which he presents to rapt audiences as dispatches from the front ranks of science, make the top tier of scientists roll their eyes or get very angry. “In my opinion, what he’s doing is the modern equivalent of phrenology,” says Jeffrey Lieberman, APA presidentelect, author of the textbook “Psychiatry” and chairman of Psychiatry at Columbia University College of Physicians and Surgeons. (Phrenology was the pseudoscience, popular in the early 19th century, that said the mind was determined by the shape of the skull, particularly its bumps.) “The claims he makes are not supported by reliable science, and one has to be skeptical about his motivation.” “I think you have a vulnerable patient population that doesn’t know any better,” says M. Elizabeth Oates, chair of the Commission on Nuclear Medicine, Board of Chancellors at the American College of Radiology, and chair of the department of radiology at the University of Kentucky.
“A sham,” says Martha J. Farah, director of the Center for Neuroscience & Society at the University of Pennsylvania, summing up her thoughts on one of Amen’s most recent scientific papers. “I guess we’re all amateurs except for him,” says Helen Mayberg, a psychiatry, neurology and radiology professor at Emory School of Medicine and one of the most respected researchers into depression and brain scanning. “He’s making claims that are outrageous and not supported by any research.” “I can’t imagine clinical decisions being guided by an imaging test,” says Steven E. Hyman, former director of the National Institute of Mental Health and current director of the Stanley Center for Psychiatric Research at the Broad Institute of MIT and Harvard.
The APA, in fact, has twice issued papers that dispute “claims being made that brain imaging technology ... was useful for making a clinical diagnosis and for helping in treatment selections.” The most recent paper was the work of 12 doctors who spent three years assessing the latest research. The summary: “There are currently no brain imaging biomarkers that are currently clinically useful for any diagnostic category in psychiatry.”
Four years ago, Robert Burton, the author and former associate chief of the department of neurosciences at the University of California at Mount Zion Hospital, wrote a harsh article on Salon.com about Amen’s work. The headline was “Brain Scam.” When recently told that Amen was still in business and grossed $20 million last year, Burton asked for the dollar figure to be repeated. “Oh, my God,” he said. “Just oh, my God. At some point this gets to be obscene — that’s just my bias — but oh, my God.”
To read the entire article from The Washington Post, click here.
In 2010, concerns about Dr. Amen and the "brain scam industry" reached a boiling point. In The American Journal of Psychiatry, my colleague Dr. Bryon Adinoff wrote the following:
"Dr. Amen claims that numerous psychiatric illnesses can be diagnosed and treatments prescribed based on resting single photon emission computerized tomography (SPECT) images. Dr. Leuchter correctly points out the absence of empirical data to support the claims of Dr. Amen. Several years ago, following conversations with Dr. Amen on how to address such concerns, the Brain Imaging Council of the Society of Nuclear Medicine offered Dr. Amen the opportunity to submit his analyses of a blinded set of SPECT scans (to have been prepared by the Brain Imaging Council) to determine how effective his technique is at correctly diagnosing subjects. Although this proposed study could have provided support for his approach, the offer was declined. Nevertheless, for more than two decades, Dr. Amen has persisted in using scientifically unfounded claims to diagnose and treat patients (over 45,000 by his own count).
"There are several dangers to patients that can accrue from this approach: 1) patients (including children) are administered a radioactive isotope without sound clinical rationale; 2) patients pursue treatments contingent upon an interpretation of a SPECT image that lacks empirical support; and 3) based on a presumed diagnosis provided by Dr. Amen's clinics, patients are guided toward treatment that may detract them from clinically sound treatments.
"Just as serious is the danger to our field. It is likely that, within the next decade, Dr. Amen's claims will be realized in that psychiatrists will enjoy the ability to diagnose and prescribe treatments based, in part, upon neuroimaging findings. Unfortunately, if previously led astray by unsupported claims, patients and their doctors may be less inclined to utilize scientifically proven approaches once these are shown in the peer-reviewed literature to be effective.
"It is therefore incumbent upon all of us to monitor and regulate our field. We encourage physicians to remain vigilant of unproven approaches practiced by our peers and to immediately report these trespasses to their state medical boards."
What the reader should understand is that Dr. Amen, like many promoters of fraudulent "cures," appeals to people who are vulnerable to snake-oil promotions and great salesmanship. He has even hornswoggled fellow entrepreneurial genius Rick Warren, best known for The Purpose Driven Life, and pastor of the Saddleback Church in California. Warren designated Amen as official guru for health and nutrition at his mega-church.
Few top researchers and scientists say that SPECT is anything but a research tool of limited clinical use in identifying strokes, brain injuries and the like. It is helpful in group studies, to say broad things about groups of patients, but not specific things about individual patients. And, researchers say, SPECT has largely since been surpassed by technologies such as PET and functional MRIs, which give images of far greater clarity. It’s no longer viewed as cutting edge.
The APA first debunked many of Amen’s SPECT claims in a 2005 report. In 2008, Carlat, the Tufts professor and author, went to California to test Amen’s clinic. He then wrote, in Wired Magazine, that the black-clad Amen looked “more like a Miami maitre d’ than a psychiatrist,” that the SPECT scan was “spectacularly meaningless” and that Amen’s analysis of it reminded him of a “shrewd palm reader.”
In 2010, Thomas Insel, director of the NIMH, wrote on his blog that while the technology “might be playing in prime time on some TV infomercials, brain-imaging experts say we’re not quite there yet.” Earlier this year, Anissa Abi-Dargham, a highly regarded professor of clinical psychiatry and radiology at Columbia who has done extensive work with brain imaging, spoke at an APA symposium on the limits of SPECT. She listened to Amen’s hour-long lecture there. Reached by phone recently, she said: “Had I known what this was, I would have never agreed to be part of it. It was not a scientific debate. It was propaganda for his clinics.”
No major research institution takes his SPECT work seriously, none regards him as “the number one neuroscience guy,” and his revelations, which he presents to rapt audiences as dispatches from the front ranks of science, make the top tier of scientists roll their eyes or get very angry. “In my opinion, what he’s doing is the modern equivalent of phrenology,” says Jeffrey Lieberman, APA presidentelect, author of the textbook “Psychiatry” and chairman of Psychiatry at Columbia University College of Physicians and Surgeons. (Phrenology was the pseudoscience, popular in the early 19th century, that said the mind was determined by the shape of the skull, particularly its bumps.) “The claims he makes are not supported by reliable science, and one has to be skeptical about his motivation.” “I think you have a vulnerable patient population that doesn’t know any better,” says M. Elizabeth Oates, chair of the Commission on Nuclear Medicine, Board of Chancellors at the American College of Radiology, and chair of the department of radiology at the University of Kentucky.
“A sham,” says Martha J. Farah, director of the Center for Neuroscience & Society at the University of Pennsylvania, summing up her thoughts on one of Amen’s most recent scientific papers. “I guess we’re all amateurs except for him,” says Helen Mayberg, a psychiatry, neurology and radiology professor at Emory School of Medicine and one of the most respected researchers into depression and brain scanning. “He’s making claims that are outrageous and not supported by any research.” “I can’t imagine clinical decisions being guided by an imaging test,” says Steven E. Hyman, former director of the National Institute of Mental Health and current director of the Stanley Center for Psychiatric Research at the Broad Institute of MIT and Harvard.
The APA, in fact, has twice issued papers that dispute “claims being made that brain imaging technology ... was useful for making a clinical diagnosis and for helping in treatment selections.” The most recent paper was the work of 12 doctors who spent three years assessing the latest research. The summary: “There are currently no brain imaging biomarkers that are currently clinically useful for any diagnostic category in psychiatry.”
Four years ago, Robert Burton, the author and former associate chief of the department of neurosciences at the University of California at Mount Zion Hospital, wrote a harsh article on Salon.com about Amen’s work. The headline was “Brain Scam.” When recently told that Amen was still in business and grossed $20 million last year, Burton asked for the dollar figure to be repeated. “Oh, my God,” he said. “Just oh, my God. At some point this gets to be obscene — that’s just my bias — but oh, my God.”
To read the entire article from The Washington Post, click here.
In 2010, concerns about Dr. Amen and the "brain scam industry" reached a boiling point. In The American Journal of Psychiatry, my colleague Dr. Bryon Adinoff wrote the following:
"Dr. Amen claims that numerous psychiatric illnesses can be diagnosed and treatments prescribed based on resting single photon emission computerized tomography (SPECT) images. Dr. Leuchter correctly points out the absence of empirical data to support the claims of Dr. Amen. Several years ago, following conversations with Dr. Amen on how to address such concerns, the Brain Imaging Council of the Society of Nuclear Medicine offered Dr. Amen the opportunity to submit his analyses of a blinded set of SPECT scans (to have been prepared by the Brain Imaging Council) to determine how effective his technique is at correctly diagnosing subjects. Although this proposed study could have provided support for his approach, the offer was declined. Nevertheless, for more than two decades, Dr. Amen has persisted in using scientifically unfounded claims to diagnose and treat patients (over 45,000 by his own count).
"There are several dangers to patients that can accrue from this approach: 1) patients (including children) are administered a radioactive isotope without sound clinical rationale; 2) patients pursue treatments contingent upon an interpretation of a SPECT image that lacks empirical support; and 3) based on a presumed diagnosis provided by Dr. Amen's clinics, patients are guided toward treatment that may detract them from clinically sound treatments.
"Just as serious is the danger to our field. It is likely that, within the next decade, Dr. Amen's claims will be realized in that psychiatrists will enjoy the ability to diagnose and prescribe treatments based, in part, upon neuroimaging findings. Unfortunately, if previously led astray by unsupported claims, patients and their doctors may be less inclined to utilize scientifically proven approaches once these are shown in the peer-reviewed literature to be effective.
"It is therefore incumbent upon all of us to monitor and regulate our field. We encourage physicians to remain vigilant of unproven approaches practiced by our peers and to immediately report these trespasses to their state medical boards."
Child Development and Brain Health
In teaching medical students about psychiatry, I say that there are two key factors that influence how an individual fares in life. One factor is biological vulnerability, and the other factor is developmental opportunity. A person may be born with a genetically influenced condition like dyslexia, or a genetic vulnerability to addiction (alcoholism, for example, tends to run in families). Someone with biological vulnerability may, however, do quite well if life is filled with developmental opportunity. A person who grows up in a stable family, who attends good schools, and who gets a good job has a life rich in developmental opportunities that may ultimately enable them to overcome the biological vulnerability.
Someone with dyslexia may attend schools that recognize the deficit and help the child learn to read well; or they may have the help of a skilled educational psychologist who can work the magic and overcome the learning differences. On the other hand, someone who grows up in less fortunate circumstances, like living in poverty or suffering a broken home, may do very well if they are biologically resilient and strong. Problems arise, however, when some suffers biological vulnerability as well as a life short on developmental opportunity. When we see the chronically mentally ill, we often see the overlap of these two conditions.
New research suggests that family income, and to a lesser degree parental education, are associated with brain structure differences in children and young adults. Focusing on brain regions critical for language, memory, and executive function in participants aged three to 20 years, scientists found that small differences in income were associated with relatively large differences in brain surface area in young people from the lowest-income families. This effect was smaller in higher-income families. Higher income was also associated with better performance in tests of cognitive ability. Increased levels of parental education were also related to increased brain surface area, although this effect was smaller when compared to the influence of income.
Although these study results do not suggest that low-income children have poor cognitive function, they indicate that interventions to reduce family poverty may help reduce socioeconomic disparities in child development and achievement. The full text of the findings can be found here.
Someone with dyslexia may attend schools that recognize the deficit and help the child learn to read well; or they may have the help of a skilled educational psychologist who can work the magic and overcome the learning differences. On the other hand, someone who grows up in less fortunate circumstances, like living in poverty or suffering a broken home, may do very well if they are biologically resilient and strong. Problems arise, however, when some suffers biological vulnerability as well as a life short on developmental opportunity. When we see the chronically mentally ill, we often see the overlap of these two conditions.
New research suggests that family income, and to a lesser degree parental education, are associated with brain structure differences in children and young adults. Focusing on brain regions critical for language, memory, and executive function in participants aged three to 20 years, scientists found that small differences in income were associated with relatively large differences in brain surface area in young people from the lowest-income families. This effect was smaller in higher-income families. Higher income was also associated with better performance in tests of cognitive ability. Increased levels of parental education were also related to increased brain surface area, although this effect was smaller when compared to the influence of income.
Although these study results do not suggest that low-income children have poor cognitive function, they indicate that interventions to reduce family poverty may help reduce socioeconomic disparities in child development and achievement. The full text of the findings can be found here.