Mindfulness Meditation Improves Health
In one study conducted at the Wake Forest Baptist Medical Centre in North Carolina, scientists found that doing meditation daily for a few minutes could relieve pain better than a powerful pain relieving medication.
What is meditation? If you've followed my blog here (or if you browse earlier posts) you know that my approach to meditation is quite simple and straightforward. Although I have studied theology and philosophy seriously, including the great religions, I do not see meditation through the lens of religion. Like contemplative prayer, however, meditation has the capacity to soothe, calm, and relax the mind, and the most challenging aspect of meditation is simply to practice on a daily basis.
Meditation is the simple practice of making the mind calm, and silent, and bringing your thoughts to one point. In other words, meditation can be defined as making mind free from agitation, turning attention away from distracting thoughts and focusing on the present moment. Some individuals incorporate meditation as part of religious practice, and others do not. Yoga, for example, is one approach to meditation that has spiritual roots, and the same is true of contemplative prayer in Christian and Jewish traditions. Zen meditation, deriving from Buddhism, also has spiritual aspects.
Christian writer Phil Fox Rose says, "The promise of a devoted spiritual life, of which meditation is an invaluable part, is serenity...that in everyday life you will not be anxious, restless or irritable; and that in good times you will be fully alive to enjoy them."
After practicing meditation for even a few weeks, what many people notice is that mindfulness becomes a part of everyday life. In other words, we become more mindful in every activity. We focus more clearly, we think and speak more in terms of the present moment, and we act with greater compassion and clarity.
Meditation produces many benefits. I have noticed that my meditation practice improves concentration, strengthens the mind and leads to multiple health benefits: lowering blood pressure, reducing emotional distress , diminishing anxiety attacks, and improving my relationships.
The Wake Forest study now shows that meditation each day could be better in relieving pain than taking morphine. Similar studies at Duke and Harvard point to similar findings.
In their study, the lead researcher, Dr. Fadel, examined the brain scans of individuals who had been trained to use relaxation and breathing techniques to cope with the pain. After studying the brain scans, his team noticed that the study subjects who meditated regularly had calmer brain scans. They saw a 27 percent reduction in pain intensity and 44 percent less emotional pain in group of volunteers who actually practiced mindfulness meditation.
Along with many others, I believe that such findings prove that mindfulness meditation can produce different patterns of brain activity to suppress the feeling of pain.
Based on the study results, the scientists believe 20-minute a day meditation practice could be added to conventional pain relief methods for better and quicker relief. The study focused on volunteers who were pain free, so the question remains as to whether individuals with more serious pain problems can achieve similar results. The study findings are reported in the Journal of Neuroscience.
Another study from the Department of Psychiatry at Duke University Medical Center shows that mindfulness meditation can protect against depression. There are now hundreds of scientific papers on mindfulness. A Harvard Medical School study showed promising results in pain relief: "Recently, it has been demonstrated that pain can also be attenuated by mindfulness….Mindfulness practitioners and controls received unpleasant electric stimuli in the functional magnetic resonance imaging scanner during a mindfulness and a control condition. Mindfulness practitioners, but not controls, were able to reduce pain unpleasantness by 22% and anticipatory anxiety by 29% during a mindful state."
Let me know if you discover new findings in this exciting area of research!
What Are Marijuana "Dabs"?
A dab usually refers to a dose of concentrate that is heated on a hot surface, usually a nail, and then inhaled through a "dab rig." It doesn't sound so controversial in those terms, but “blasting dabs” has become a dividing point within the community both because of the intense high that it produces and for the image that it presents to outsiders.

A Dab Rig Sold Online
What are Dabs and How are They Made?
Dabs are concentrated doses of cannabis that are made by extracting THC and other cannabinoids using a solvent like butane or carbon dioxide, resulting in sticky oils also commonly referred to as wax, shatter, budder, and butane hash oil (BHO). While it's possible to extract non-psychoactive compounds like CBD, THC is what's behind the potent effects of dabs, making them the fastest and most efficient way to get really, really medicated. Terpenes, or the aromatic oils that give cannabis flavor, can also be extracted, although it can be difficult to preserve these volatile compounds in the extraction process.


From http://leafly.com
What are the Concerns Surrounding Dabbing?
Here's what the Leafly website says about dabbing: "Let’s start with the bad news first: dabbing can be dangerous. Actually, it’s the extraction that can be dangerous.The process can be tricky, but thanks to online forums and videos, many amateur "scientists" think they have mastered the technique enough to try it on their own. In cases when things go well, the product is probably still pretty poor. When things go bad, houses blow up. When I worked out in rural Texas, people were getting blown up when cooking methamphetamine in their kitchens. Today, there are other ways (like extracting cannabis oil) that apparently can get you blown up as well.
"Another side effect of these home extraction experiments is “dirty” oil that may contain chemical contaminants that could present health hazards to consumers. If the concern is butane, the dangers are most likely minimal since it already occurs in everyday products such as scent and flavor extracts. Whether or not the equipment used in the extraction process is adding additional contaminants is a more viable issue. When done correctly, these extras can be avoided, so as is the case with growing cannabis, it’s best to leave it to those who know what they’re doing.
"One of the most unsettling facts about dabs is that thanks to the super-concentrated power of BHO, for the first time it seems possible to “overdose” on cannabis. While still not lethal, taking more than your personal limit of dabs can lead to uncomfortable highs and, in some cases, passing out. After all of the chanting that “you can’t overdose on marijuana,” concentrates could be undermining advocates’ message of safety. There have also been reports of more intense withdrawal symptoms for dabbers, but again, the information is limited."
For more on recent research on potential problems with marijuana, see my previous post (scroll down here on the blog) "Update on Marijuana Research."

Pain Pill Addiction: Basics
Breaking free of prescription drug abuse takes much more than willpower. As I often say, "You have to do it yourself, but you can't do it alone." There are individuals who claim to have "kicked" or achieved abstinence without any help, but I don't know many of them. Early on, before dependency sets in, it's possible to recognize the problem and stop using narcotics. Once dependence sets in, though, it's not so easy.
Fortunately, medications and counseling can improve the chances of success. Newer drugs like buprenorphine (sometimes combined with naloxone) and naltrexone and traditional therapies like methadone and 12-step programs, are helping thousands of people stay on the road to recovery.
Physical Dependence and Detoxification
Narcotic addiction leads to real changes in certain areas of the brain. Prescription drug addiction alters the circuits responsible for mood and "reward" behaviors.
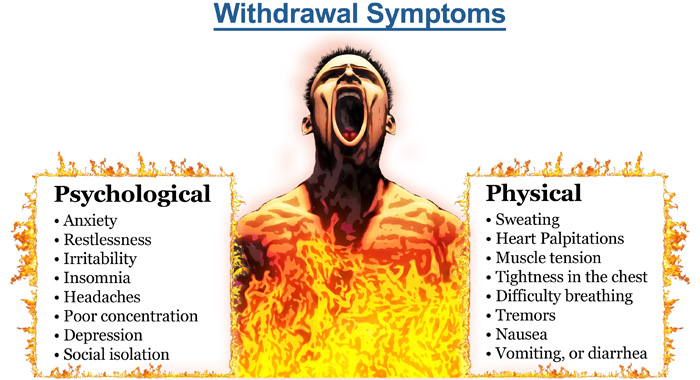
In addition, long-term prescription drug abuse affects virtually all the systems in the body. Cutting off the supply abruptly leads to opioid withdrawal symptoms.
Symptoms of opioid withdrawal include:
- Craving for drugs
- Diarrhea
- Large pupils
- Yawning
- Abdominal pain
- Chills and goose bumps (the origin of the phrase "cold turkey")
- Nausea and vomiting
- Body aches
- Agitation and severe negative moods
A list of symptoms doesn't capture the agony of opioid withdrawal.
The syndrome is intensely unpleasant, and people will do almost anything to avoid it.
Opioid withdrawal lasts from hours to several days -- and sometimes weeks -- depending on how long and how much a person has used their drug of choice. After the intense initial symptoms subside, some physical and mental discomfort may persist for weeks.
Medications for Opioid Withdrawal
Opioid withdrawal is difficult to endure, and is a major reason for relapse and continued prescription drug abuse. Medications are used to prevent symptoms of opioid withdrawal during detox, easing the person out of physical dependence:
Methadone is a long-acting opioid drug. It activates the same opioid receptors as narcotics, effectively eliminating withdrawal symptoms. Providing the correct dose of methadone prevents opioid withdrawal symptoms and eases drug craving but it does not provide the euphoria. The dose can be slowly tapered off, freeing the person from physical dependence without withdrawal symptoms. Methadone is the most effective known treatment for narcotic addiction.
Buprenorphine and Naloxone (Suboxone) is a newer combination drug that helps for detox from prescription opioid addiction. Buprenorphine activates opioid receptors, reducing drug craving and preventing withdrawal. Naloxone helps prevent misuse of the medication.
Clonidine is a blood pressure medicine that acts on the brain. Clonidine reduces the effects of the "fight or flight" response, which is over-activated during opioid withdrawal. However, clonidine does nothing to reduce drug craving, and is mostly ineffective when used alone.
"Rapid detox" programs claim to accelerate the process of detox and opioid withdrawal by giving large doses of opioid blocking drugs. Some programs place an addict under general anesthesia during the detox process. These programs have not proven to be more effective than traditional methods of detox, and may be more dangerous.
Maintenance Therapy After Detox
Completing detox subdues the physical effects of narcotic addiction and opioid withdrawal. But experts say psychological and social factors are the main drivers that push addicts back to using. Stress and situations that remind the brain of the drug's pleasure are common triggers.
When drug cravings strike, they can be impossible to resist. Most people who go through detox and short-term counseling will relapse to prescription drug abuse.
Studies show that the chances of beating narcotic addiction are better with long-term maintenance therapy with either methadone or buprenorphine paired with naloxone (Zubsolv, Bunavail, Suboxone) . These drugs are used during the maintenance phase of treatment. People on these drugs are still opioid-dependent, but they are often freed from their destructive drug addiction. They can return to work, drive without impairment, and function normally in society. Naloxone has also been combined with oxycontin ( Targiniq ER ) to deter abuse by snorting or injecting the drug. A person can still become addicted by taking it orally, however.
Methadone is the best-studied, most effective method of recovery from narcotic addiction. Suboxone, while newer, has gained wide acceptance as maintenance therapy.
Some people have a high rate of relapse when maintenance therapy is stopped, and so they remain on the medicines for decades. In others, maintenance therapy is tapered off over months to years.
Naltrexone (ReVia, Vivitrol) is an opiate receptor-blocking medication used in maintenance therapy for narcotic addiction. Unlike methadone and Suboxone, naltrexone does not activate receptors at all, so it does not reduce opioid withdrawal or craving. However, because naltrexone blocks opiate receptors, a person won't get high if he or she uses drugs while taking the medicine. The drug is usually ineffective by itself, because people can simply stop taking it and get high shortly after.
Counseling and 12-Step Programs
Narcotics Anonymous (NA) is an international network of community-based meetings for those recovering from drug addiction. Modeled after Alcoholics Anonymous (AA), NA is a 12-step program with a defined process for overcoming narcotic addiction.
NA is an abstinence-based program. In principle, NA is opposed to the use of maintenance therapy. Methadone Anonymous is a 12-step program that acknowledges the value of methadone or Suboxone in recovery from narcotic addiction. Methadone Anonymous has caught on in California, but I don't know much about meetings in Texas. If you have information about Methadone Anonymous meetings, contact me.
Most of us who are experts in the field recommend participation in a 12-step program or other form of counseling. Therapy can take place as an outpatient, or in a residential facility. I discuss the value of 12 Step Programs on my FAQ page.
Update on Marijuana Research
According to a recent analysis presented at the 2015 Meeting of the American Chemical Society, the amount of THC in samples from marijuana sold in Colorado are reaching 30 percent. Three major patterns have emerged over the past few months since Andy LaFrate, Ph.D., and his lab began testing marijuana samples. Those patterns concern potency, amounts of a substance called CBD and contaminants in the products.
“As far as potency goes, it’s been surprising how strong a lot of the marijuana is,” LaFrate says. “We’ve seen potency values close to 30 percent THC, which is huge.” LaFrate is the president and director of research of Charas Scientific, one of eight labs certified by Colorado to do potency testing.
THC is an abbreviation for tetrahydrocannabinol, which is the psychoactive compound in the plant. He explains that three decades ago, THC levels were well below 10 percent. Its content has tripled in some strains because producers have been cross-breeding them over the years to meet user demands for higher potency, he says.
But an unexpected consequence of this breeding has occurred, says LaFrate. Many of the samples his lab has tested have little to no cannabidiol, or CBD. CBD is a lesser known compound in marijuana that is of increasing interest to medical marijuana proponents. Researchers are investigating CBD as a treatment for schizophrenia, Huntington’s disease and Alzheimer’s disease. It is also being considered for anxiety and depression. But unlike THC, CBD doesn’t get people high — that’s a key trait for many people who are wary of buzz-inducing drugs and for potential medical treatments for children. As for recreational users, the lack of CBD in marijuana means that many of the hundreds of strains they select from could in actuality be very similar chemically, according to LaFrate.
"What we have today is not the weed we used to smoke in the 1960's."
In a recent report researchers found that the concentration of THC sold on the streets in Denmark has tripled to an average of 28 percent in the last 20 years.
Attitudes toward marijuana are also rapidly changing. In the 1960s surveys found a mere 12 percent supported marijuana legalization—now, more than 50 percent are in favor. Over the past decade recreational/medicinal use of cannabis was legalized in the District of Columbia as well as in Alaska, Colorado, Oregon and Washington State; 19 other states also permit the use of the drug for medical purposes. As more states and countries, such as Canada and the U.K., consider following suit, advocates and critics are engaging in heated debates about the potential risks and rewards—particularly in light of the increasing prevalence of highly potent marijuana. But the evidence is nebulous—even within the scientific community, there is lack of consensus about how much harm marijuana can do to users’ brains and mental health.
In addition to THC, the other major component of marijuana that has caught the attention of researchers is cannabidiol (CBD), which scientists have linked to antipsychotic properties. Not only do THC and CBD have opposing effects, cannabis with higher THC content tends to contain lower amounts of CBD. “The relationship between CBD and THC is unique, in that the biological process required to make THC antagonizes the generation of CBD,” says Matthew Hill, a cannabinoid neuropharmacologist at the University of Calgary.
Damage to the brain?
In an article published last month in Psychological Medicine, researchers conducted a neuroimaging study to assess the effects of cannabis use on the corpus callosum, the largest collection of white matter in the brain containing fibers that facilitate communication between the two hemispheres. They found that this structure was negatively affected in those who used high potency cannabis—strains high in THC and low in CBD—compared with those who used lower strength bud or did not use at all. Moreover, the changes were similar in both those with and without previous episodes of psychosis. However, the researchers assert that they did take other drug usage into account.
Previous studies have demonstrated the importance of these confounding factors when interpreting marijuana’s effects on the brain. For example, a 2014 study in The Journal of Neuroscience reported that marijuana use was associated with changes in brain structures associated with reward processing. This effect was dose-dependent, meaning the more cannabis someone used, the more changes became apparent in their brains. In a subsequent study, published in 2015 in the same journal, another group of researchers found that once variables such as alcohol use, gender and age were controlled for, the differences between users and nonusers disappeared.
Marijuana madness?
In a study published earlier this year in Lancet Psychiatry the same group of researchers at King’s College found that using cannabis, and THC specifically, can produce acute psychotic symptoms, and some researchers suggest it increases the risk of developing schizophrenia. The link between marijuana and psychosis, however, has been a matter of heated debate in the scientific community. Researchers have argued that there are sufficient grounds to doubt the causality of this link. There are two alternative possibilities: being predisposed to schizophrenia may increase the likelihood for cannabis use or a third variable may make it more likely for people to use marijuana and develop schizophrenia. For example, previous studies have suggested that schizophrenia and cannabis share both genetic and demographic risk factors, such as low socioeconomic status.
Critics also point to the fact that all the studies to date have been correlational. But this does not immediately dismiss the possibility that causation is possible. After all, although there was a strong correlational link between smoking and cancer, it took a study of more than 30,000 British doctors to confirm causality.
According to Haney, the odds ratio—the likelihood that an exposure will lead to a certain outcome—of marijuana causing psychosis are much lower than those for smoking and cancer. “There is also an association with tobacco smoking and schizophrenia that is much stronger [than cannabis use],” Haney says. “If this relationship is causal, it is a tiny effect, which might explain why there hasn't been a dramatic upsweep in rates of schizophrenia in recent years.”
Both Haney and Evins agree that it is biologically plausible that marijuana, particularly at a young age, could increase the likelihood of negative psychiatric outcomes. The developing brain has an abundance of cannabinoid type 1 (CB1) receptors, where THC binds to exert its effects, in the prefrontal cortex, a key brain area impacted by schizophrenia. “I don't think it's a good idea for young children to be smoking marijuana at all because of their developing brains but I am extremely cautious about pinning it all on marijuana when there is a potential for many other explanations,” Haney says.
To truly determine whether marijuana causes such effects, scientists would need to track changes that occur in a large number of individuals before and after they use a drug over a long period of time. An effort to conduct this type of study is currently underway—the National Institutes of Health recently funded the multicenter Adolescent Brain Cognitive Development Study, which plans to recruit 10,000 children before they start drug use, and follow them for 10 years to assess the short-and long-term effects of using marijuana, tobacco and other drugs.
Teenagers and young adults at risk?
Cannabis has been found to impair cognitive functions such as memory and is increasingly being considered an addictive substance, especially in adolescents. There are still many questions that remain to be answered but strict regulation and lack of funding pose large barriers to conducting the required studies. The U.S. Drug Enforcement Administration still classifies marijuana in its most restrictive “Schedule I” category, which puts tight regulations on researchers who want to study its effects.
A New Zealand study found that persistent cannabis users show neuropsychological decline from childhood to midlife. These scientists found that frequent and persistent marijuana use starting in adolescence was associated with a loss of an average of 8 IQ points measured in mid-adulthood. Significantly, in that study, those who used marijuana heavily as teenagers and quit using as adults did not recover the lost IQ points.
Users who only began using marijuana heavily in adulthood did not lose IQ points. These results suggest that marijuana has its strongest long-term impact on young users whose brains are still busy building new connections and maturing in other ways. The endocannabinoid system is known to play an important role in the proper formation of synapses (the connections between neurons) during early brain development, and a similar role has been proposed for the refinement of neural connections during adolescence. If confirmed by future research, this may be one avenue by which marijuana use during adolescence produces its long-term effects. (For details see: Meier MH, Caspi A, Ambler A, et al. Persistent cannabis users show neuropsychological decline from childhood to midlife. Proc Natl Acad Sci USA. 2012;109:E2657-2664.)
The ability to draw definitive conclusions about marijuana’s long-term impact on the human brain from past studies is often limited by the fact that study participants use multiple substances, and there is often limited data about the participants’ health or mental functioning prior to the study. Over the next decade, the National Institutes of Health is planning to fund a major longitudinal study that will track a large sample of young Americans from late childhood (before first use of drugs) to early adulthood. The study will use neuroimaging and other advanced tools to clarify precisely how and to what extent marijuana and other substances, alone and in combination, affect adolescent brain development.
Scientists agree the highly potent marijuana may be better to avoid. Aside from potential long-term harm, receiving a high dose of THC can be especially risky for first-time users who are more likely to experience adverse effects such as panic or anxiety attacks. But even knowing the potency of a product, consumers might not always get what they ask for.
Because of competing laws at the state and federal level, the quality of regulation varies largely between states and regions. Although THC potency labeling is mostly required for both medical and recreational products, it is not always accurate—a study published this June in JAMA The Journal of the American Medical Association revealed that of the 75 edible marijuana products (from 47 different brands) researchers assessed only 17 percent accurately labeled their THC content.
The article states: "Edible cannabis products from 3 major metropolitan areas, though unregulated, failed to meet basic label accuracy standards for pharmaceuticals. Greater than 50% of products evaluated had significantly less cannabinoid content than labeled, with some products containing negligible amounts of THC. Such products may not produce the desired medical benefit.
"Other products contained significantly more THC than labeled, placing patients at risk of experiencing adverse effects.5,6 Because medical cannabis is recommended for specific health conditions, regulation and quality assurance are needed.
"A limited number of cities, dispensaries, and products were included. Because no source lists all dispensaries, and many products are not labeled with cannabinoid content, a true random sample was not possible and the results may not be generalizable. However, this study illustrates the variability in label accuracy for edible cannabis products within 2 of the largest medical cannabis markets in the United States."
Across labs and in homes, marijuana remains a highly debated issue. Marijuana is an extremely polarizing topic among scientists, as these articles demonstrate. My own view is that marijuana is not likely to cause someone to suffer a schizophrenic illness, but clearly what we have today is not the weed we smoked in the 1960's.
Random Facts on Happiness
I've collected various facts about happiness. Here are a few of them, with a little help from my friends at WebMD:
Californians are not terribly happy. Out of 51 slots, California ranks No. 46 on the happiness scale. Surprisingly, New York and California do badly in the happiness ranking. Researcher Andrew Oswald of the University of Warwick in Coventry, England, says, "Many people think these states would be marvelous places to live, but the problem is that if too many individuals think that way, they move into those states, and the resulting congestion and house prices make it a non-fulfilling prophecy." So where is the No. 1 place brimming with happiness, you ask? Louisiana!
It's a fact: People are happier, less stressed, and feel better about themselves after age 50! A recent survey of more than 340,000 people showed overall feelings of well-being improve as people pass middle age. Negative emotions such as stress and anger decline after the early 20s, and people over 50 worry less than younger folks. Researchers say it may be as simple as this: With age comes increased wisdom and emotional intelligence.
In terms of happiness, a boost in your mood is linked to the release of serotonin, endorphins -- your body’s "feel good" chemicals -- and oxytocin, also known as the "love/comfort/compassion" hormone. Tryptophan helps your body make serotonin, so it’s linked to feeling good, too.
Good news for folks whose bedrooms have more activity than their bank accounts: Research shows that sex is better for your happiness than money. Overall, the happiest folks are those getting the most sex: married people, who report 30% more between-the-sheet action than single folks.
Dopamine is a feel-good chemical that’s involved in pleasure. A study found that when people listened to music, their brains released more dopamine. In fact, even just thinking about listening to music caused the dopamine to start flowing. The researchers think this might explain why music -- from Beethoven’s Fifth to Adele’s "Rolling in the Deep" -- has been such a big part of human history.
Having a positive outlook doesn't mean you never allow yourself to feel sad. "Happiness is not the absence of sadness," says David Spiegel, MD, medical director of the Center for Integrative Medicine at Stanford University School of Medicine. It is not a stiff upper lip or the pop psychology mantra, intoning "always stay upbeat" no matter what. "Phony happiness is not good." By suppressing sadness, you suppress other, more positive emotions, as well, he says. So people who try to suppress emotions actually become more anxious and depressed.
Sure, pleasure is great and you need plenty of it, though there is more to happiness than racking up pleasurable experiences. Psychologists studying the effects of positive emotions say gratitude can boost our sense of happiness if we turn it into a conscious and regular practice. Feeling gratitude, they say, is something you do (such as expressing gratitude or keeping a gratitude journal), not something you wait for!
Some studies have found that laughter may boost infection-fighting antibodies and immune cells in the body. And when scientists at the University of Maryland studied the effects on blood vessels when people were shown either comedies or dramas, they found that the people who watched dramas tended to tense up, restricting blood flow. The people who watched comedies had normal blood flow.
Recognizing Bullshit!
Our lecture was designed to show that psychiatry, like many other professions, engages in "a great deal of bullshitting when it comes to human nature and personal experience." Needless to say, the talk stirred a bit of controversy, and the medical school was not quite sure how to advertise the event.
The concept of "bullshit," however, is quite relevant in psychiatry and philosophy, as Professor Harry Frankfurt has pointed out in his essay, "On Bullshit," which is included in his wonderful book of essays, The Importance of What We Care About. That book, as much as any other, has influenced my life and work for many years. I refer to it in a brief paper published in the Journal of Philosophy, Psychiatry, and Psychology.
Dr. David Scales has written a terrific article published on WBUR's CommonHealth, and I really got a kick out of this, so I offer it here in full. In the online article, the editors had to take out the word "bullshit" and replace it with BS, so I have taken the liberty of using the actual word, for obvious reasons.
Deep? Or Pseudo-Profound Bullshit? Psychologists Explore Why Some Can’t Tell
What do you think of the following sentences?
“The universe is the wisdom of objective external reality.”
“Experiential truth embraces the expansion of actions.”
“Death is only possible in intrinsic possibilities.”
Are they profound wisdom? Or are they bullshit? If you thought they were profound, you might need your bullshit detector checked.
Created from the website wisdomofchopra.com, this “wisdom” was generated by randomly putting together words found in the tweets of Deepak Chopra, the physician and author.
Who is more likely to see such bullshit as profound? And why? These are the questions that motivated Gordon Pennycook, a psychology PhD student at the University of Waterloo in Ontario, Canada, and his colleagues to publish a paper this week called “On the reception and detection of pseudo-profound bullshit.” (They spelled out the full word, which academic psychology allows but the AP Stylebook we use does not.)
The researchers took quotes like those above and tested whether people could see pseudo-profound statements for what they were — bullshit. Their findings suggest that people with higher intelligence and better critical-thinking skills are likeliest to detect bullshit. And more than one-quarter of the population they studied were particularly prone to buying in to it — and to holding, shall we say, “alternative” beliefs on topics from medicine to magic.
At first, this may seem like -- you know -- bullshit, but Gordon Pennycook is a real person. [Yes, Pennycook is his real name, despite its similarity to “poppycock.”] And if you wonder whether studying susceptibility to bullshit is important, just consider the possible effects on everything from votes in next year’s election to purchases of purported cure-all supplements.
The paper, published in the journal Judgment and Decision Making, is a remarkable study, not only in profane language — using the word bullshit about 200 times — but also in finally applying empirical analysis to the study of bullshit. Much has been written about it previously, but mostly just musings on the topic: “bullshit about bullshit,” Pennycook joked.
Bullshit hasn’t always gone by that name. It has been variously called crap (Hemingway), humbug, mumbo-jumbo, hot air, gobbledygook, hogwash, claptrap, woo-woo, baloney (Carl Sagan), bunk, poppycock or Orwellian doublespeak. “The fact that we have so many words for bullshit shows how pervasive it is,” Pennycook said.
What is it exactly? First defined by Dr. Harry Frankfurt, author of the best-selling book “On Bullshit,” it is different from lying, in which people deliberately manipulate or subvert the truth. Instead, bullshit statements are designed to sound impressive but have no regard for the truth.
As the authors of the study note, “it attempts to impress rather than to inform; to be engaging rather than instructive.” Think politics, advertising or bureaucratese. As Carl Sagan put it, “credulous acceptance of baloney can cost you money…but it can be much more dangerous than that, and when governments and societies lose the capacity for critical thinking, the results can be catastrophic.”
What Makes Us Susceptible?
We all think that we have highly attuned bullshit detectors, probably from years of listening to politicians. But the key questions that psychologists are trying to understand are: What makes some people more prone to seeing bullshit as profound? Are there personality traits, like open-mindedness or Sagan’s critical thinking, that incline someone toward being more accepting or skeptical of it?
In various experiments, the researchers asked participants to rank various short phrases from 1 to 5, giving higher numbers to more profound statements. Some statements were manufactured bullshit, like the tweets above. Some were mundane, like “Most people enjoy some sort of music.” And some were profound, like “Your teacher can open the door, but you must enter by yourself.”
“We speak of bullshit artists and spin doctors. To call it
artistry implies originality, innovation and creativity.”
– Philosopher Harry Frankfurt
Most participants could detect bullshit statements, and could easily differentiate mundane phrases from truly profound phrases. But some had difficulty weeding out the pseudo-profound from actually profound motivational statements. A full 27 percent gave bullshit statements a score of 3 or more.
What made them more prone to believing the bullshit was profound? To test that, the researchers followed the initial experiments by doing cognitive testing on the participants to assess their intelligence, and asked about spiritual leanings, views on conspiracy theories and alternative medicine.
They found that people who were less analytic and had lower cognitive ability were more prone to confuse the bullshit for the profound. That wasn’t all; those people were “more likely to hold religious and paranormal beliefs, and are more likely to endorse complementary and alternative medicine.”
In short, it looks like Carl Sagan’s intuition was right. Critical thinking may be your best defense against bullshit.
The Father Of Bullshit Studies
Why is it worth developing ways to study bullshit empirically in the lab? It’s the next step in a field that has taken off thanks to a seminal text that turned out to be a watershed: Dr. Frankfurt’s “On Bullshit“. Originally published in an obscure journal article in 1986, underground buzz led Princeton University Press to publish it as a small book in 2005. It reached No. 1 on The New York Times Bestseller List, spending 27 weeks there. Today, the book has been cited over 600 times.
“It was a concept I was using quite freely but I didn’t really know what it meant,” Dr. Frankfurt, now an emeritus professor of philosophy at Princeton University, said in a phone interview. “As an analytical philosopher, it’s my job to clarify and illuminate concepts like that.”
We need to study bullshit because we seem to have a higher tolerance for it than for lying, he argues. “We may seek to distance ourselves from bullshit, but we are more likely to turn away from it with an impatient or irritated shrug than with the sense of violation or outrage that lies often inspire,” he noted in his original article. For some reason, it doesn’t seem to violate our expectations of polite society.
Perhaps our tolerance is already explained by how we talk about it. “We speak of bullshit artists and spin doctors,” Dr. Frankfurt told me. “To call it artistry implies originality, innovation and creativity.”
The book’s unlikely success could probably be chalked up to both the ubiquity of the concept in our daily lives and its profanity. The word itself carries power. “It was very provocative to see a book by an Ivy League professor dealing with such a topic,” he told me. “I made the topic respectable in a way.”
That power to provoke also struck Pennycook. “There is force behind the word "bullshit" that implies, ‘We’re not OK with this,’ ” he said. “I think we should be forceful with our labels.”
The study authors specifically looked at “pseudo-profound bullshit.” That may sound redundant, but, as the authors note, it is only one type of bullshit. Thinking quickly, you can easily come up with other examples of bullshit. For me, the card game characterized by bluffing and “bullshitting your way through” comes to mind, and particular situations (like college, an interview or life itself.) Others have written about various types: pomposity or fanaticism, pseudoscientific nonsense or academic writing which has no regard for meaning.
To test the pseudo-profound sort, the researchers needed to be able to create bullshit— at will. It turns out, that’s the easy part. Profound-sounding but ultimately meaningless sentences are everywhere on the Internet. There’s the Twitter hashtag #cosmicconsciousness or wisdomofchopra.com. They also included quotes from the New Age Bullshit Generator, which is a load of fun.
(I hope you weren’t planning on getting anything else done today besides wasting time on fake pseudo-profound, new age tweets. You’re welcome.)
To explain how a psychology paper about bullshit ends up on a health blog: It is worth noting that the two bullshit generators for this paper were both inspired by quotations from Chopra, who is a physician. I’ve never read any of his books, so I cannot say whether his writings are bullshit, but profound-sounding misinformation is unfortunately all too common in health and medicine. Think about the late-night infomercials selling diet pills or vitamins. The wary health consumer should always be on the lookout for bullshit.
An interesting footnote: “On Bullshit” was translated into at least 16 languages. Dr. Frankfurt recalled that for some of them, like French, Russian, Portuguese and Hebrew, no exact equivalent for the term “bullshit” could be found, so they used the term “bullshit” spelled out in their own alphabet.
“I don’t understand how languages can get along without it,” he said. “It’s not as if the phenomenon is unknown to them.”
Learn About Your Brain!
Are you curious about what goes on inside your head? Every thought and action is controlled by the brain — the body’s most complex organ. The brain is divided into functional units with particular tasks, like processing visual information or responding to fearful experiences. Each of these units is made up of brain cells that work together. These cells also form connections with cells in other functional units, creating communication routes for brain signals.
Using new tools to tag and trace brain circuits, scientists are working to better understand how the human brain is organized to perform its many functions. Ongoing studies in animals and people are helping scientists recognize the many different types of brain cells and the roles they play. In addition, imaging technology is helping map brain regions responsible for specific functions and behaviors.
A great introduction to the different parts of the brain is on the Brainfacts website here. A much more detailed source for images of the brain can be seen here.
BROKEN BRAINS ADVANCE NEUROSCIENCE
In this podcast from Science Friday, science writer Sam Kean joins Ira Flatow to talk about the brain injuries that led to some of neuroscience’s biggest breakthroughs. From “H.M.,” who lost his memory during surgery, to Phineas Gage, whose grisly encounter with a tamping iron put him into high school psychology books, Kean explains how the field of neuroscience emerged from stories of brains gone awry.
AND WHAT ABOUT ADDICTIONS?
Addiction is a chronic brain disease that causes people to lose their ability to resist a craving, despite negative physical, personal, or social consequences. People seek out nicotine and alcohol, or engage in gambling, because it makes them feel good or lessens feelings of stress and sadness. Many abused drugs produce a pleasurable feeling by exciting cells in the brain’s reward center.
With repeated use, drugs can change the structure of the brain and its chemical makeup. But why can some people casually drink alcohol or smoke cigarettes, while others fight to kick the habit?
Neuroscience research, both in human and animal studies, is helping scientists identify key factors that influence susceptibility to addiction, such as a person’s genetic makeup, vulnerability to stress, and the age they start engaging in the behavior. Slowly but surely, new studies are unraveling clues about processes in the brain that influence the likelihood of drug relapse. Such insights may help improve rehabilitation programs and drive down the global cost of addiction.
Watch the video about brain chemistry and addiction here.
CASA Report on Addictions
CASA Columbia’s work for this report involved:
• A review of more than 7,000 publications
• Analyses of 5 national data sets
• Interviews with and suggestions from 176 leading experts in a broad range of fields relevant to the report
• Focus groups and a national general population survey of 1,303 adults about their attitudes and beliefs related to addiction and its treatment
• Two New York State surveys of addiction treatment providers
• An online survey of 1,142 members of professional associations involved in addiction care
• An online survey of 360 individuals with a history of addiction
• Analyses of state and federal governments’ and professional associations’ licensing and certification requirements for treatment providers
• A case study of addiction treatment in New York State and New York City
This 5-year study found that, despite the prevalence of addiction, the enormity of its consequences, the availability of effective solutions and the evidence that addiction is a disease, both screening and early intervention for risky substance use are rare, and only about 1 in 10 people with addiction involving alcohol or drugs other than nicotine receive any form of treatment.
Of those who do receive treatment, few receive anything that approximates evidence-based care. This compares with 70% to 80% of people with such diseases as high blood pressure and diabetes who do receive treatment. This report exposes the fact that most medical professionals who should be providing addiction treatment are not sufficiently trained to diagnose or treat the disease, and most of those providing addiction care are not medical professionals and are not equipped with the knowledge, skills or credentials necessary to provide the full range of effective treatments. Misunderstandings about the nature of addiction and the best ways to address it, as well as the disconnection of addiction medicine from mainstream medical practice, have undermined effective addiction treatment.
CASA Recommendations: The time has come for addiction medicine to be fully integrated into health care systems and medical practice. Health care providers, especially physicians, are our front line in disease prevention and treatment. They must understand the risk factors for addiction, screen for risky substance use and intervene when needed, and diagnose, treat and manage addiction just as they do all other diseases.
Other health care providers, including nurse practitioners, physician assistants, psychologists and social workers, are critical parts of the solution as well. We need national, evidence-based standards that stipulate who may provide addiction treatment, and core competencies for all health care providers integrated into their education and licensing requirements. We must regulate addiction treatment facilities and programs as health care providers and hold them accountable for treatment consistent with medical standards and proven practices.
Your Brain on Porn: New Findings
Porn "addiction" has been a subject of considerable debate among psychologists and in pop culture. Some argue that porn encourages sexual violence and harms relationships. Others say it may have a place in a healthy sex life.
Describing someone as a porn addict may make for catchy headlines, but in reality, there is no strong scientific research that shows such addictions actually exist. Experts say that labeling the habit of frequently viewing images of a sexual nature only describes it as a form of pathology.
“Moreover, these labels ignore the positive benefits it may hold,” said David Ley, Ph.D., a clinical psychologist. Dr. Ley is the author of a review article about the so-called “pornography addiction model,” which is published in the journal Current Sexual Health Reports.
“Pornography addiction” is not included in the recently revised Diagnostic and Statistical Manual because of a lack of scientific data.
Ley said that fewer than two in every five research articles (37 percent) about high frequency sexual behavior describe it as being an addiction. And, only 27 percent (13 of 49) of articles on the subject contained actual data, while only one related psychophysiological study appeared in 2013. Ley’s review article also highlights the poor experimental designs, methodological rigor, and lack of model specification of most studies explaining the behavior.
All told, the research found very little evidence — if any at all — to support some of the purported negative side effects of porn “addiction.” There was no sign that use of pornography is connected to erectile dysfunction, or that it causes any changes to the brains of users.
New research suggests that there's one thing porn isn't, and that's addictive.
A large study from neuroscientists at UCLA found that when people are shown erotic images, the brain's normal addiction reactions are reversed. In the brain, porn "addiction" looks the opposite of addictions like cocaine, smoking cigarettes and gambling -- and therefore should be treated with different therapies.
Typically, addicts show increased brain reactions to the object of addiction. However, the new findings, which were published this week in the journal Biological Psychology, showed that people who struggled with excessive pornography consumption had decreased brain reactions when viewing porn.
For the study, researchers recruited 122 men and women. Some of them struggled to control their pornography use, while others watched porn but said they did not have any problems with their viewing habits. The participants viewed a variety of images -- some sexual, some non-sexual -- while their brain waves were monitored using electroencephalography technology.
Using EEG, the researchers measured late positive potential (LPP) in the brain, which reflects "the intensity of an emotional response," study co-author Dr. Dean Sabatinelli explained.
"This means that their brain was not sensitized to sexual images, which is important because every other substance and behavioral addiction show sensitization in the LPP," Dr. Nicole Prause, a neuroscientist at the university and the study's lead author, told The Huffington Post in an email.
Ley's article, titled "The Emperor Has No Clothes: A Review of the ‘Pornography Addiction’ Model," offers the following summary:
"The addiction model is rarely used to describe high-frequency use of visual sexual stimuli (VSS) in research, yet common in media and clinical practice. The theory and research behind ‘pornography addiction’ is hindered by poor experimental designs, limited methodological rigor, and lack of model specification. The history and limitations of addiction models are reviewed, including how VSS fails to meet standards of addiction. These include how VSS use can reduce health-risk behaviors. Proposed negative effects, including erectile problems, difficulty regulating sexual feelings, and neuroadaptations are discussed as non-pathological evidence of learning. Individuals reporting ‘addictive’ use of VSS could be better conceptualized by considering issues such as gender, sexual orientation, libido, desire for sensation, with internal and external conflicts influenced by religiosity and desire discrepancy. Since a large, lucrative industry has promised treatments for pornography addiction despite this poor evidence, scientific psychologists are called to declare the emperor (treatment industry) has no clothes (supporting evidence). When faced with such complaints, clinicians are encouraged to address behaviors without conjuring addiction labels."
Families, Pressure, & Stress
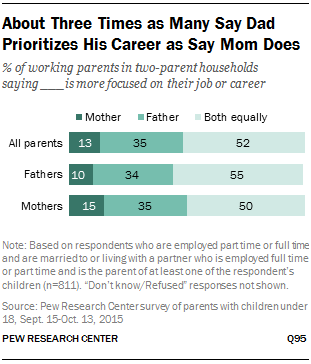
Working mothers (60%) are somewhat more likely than fathers (52%) to say it’s difficult for them to balance work and family, and this is particularly the case for mothers who work full time. In fact, one-in-five full-time working moms say balancing the two is very difficult for them, compared with 12% of dads who work full time and 11% of moms who work part time.
Overall, relatively few working parents (9%) say parenting is stressful for them all of the time. But a significant share say that parenting is stressful all or most of the time, and that sentiment is much more common among parents who say they have difficulty balancing work and family life (32% compared with 15% of those who say achieving a work-life balance is not difficult for them). In addition, four-in-ten (39%) of those who say it is hard for them to balance their responsibilities at work and at home find being a parent tiring at least most of the time; of those who say it’s not difficult for them to strike a balance, 23% say being a parent is tiring at least most of the time.
Fifty-six percent of all working parents say the balancing act is difficult, and those who do are more likely to say that parenting is tiring and stressful, and less likely to find it always enjoyable and rewarding. For example, half of those who said the work-family balance was not difficult said parenting was enjoyable all the time, compared with 36 percent of those who said balance was difficult.
In her 1989 book The Second Shift, the sociologist Arlie Russell Hochschild described the double burden employed mothers face because they are also responsible for housework and child care. Last year she said that despite some changes in society, the workplace had not changed enough to alleviate the problems. In another widely praised book, All Joy and No Fun, the journalist Jennifer Senior described how little had improved: Working parents face similar stresses, but they are now exacerbated by the expectations of modern parenthood and shared by fathers, too.
Senior draws on the psychologist Daniel Kahneman’s distinction between the “experiencing self” that exists in the present moment and the “remembering self” that constructs a life’s narrative. “Our experiencing selves tell researchers that we prefer doing the dishes — or napping, or shopping, or answering emails — to spending time with our kids. But our remembering selves tell researchers that no one — and nothing — provides us with so much joy as our children. It may not be the happiness we live day to day, but it’s the happiness we think about, the happiness we summon and remember, the stuff that makes up our life-tales.” She talks about parents’ pride in their children, not only in their accomplishments but even in their basic development as human beings, their growth into kindness and generosity. “Kids may complicate our lives,” she writes. “But they also make them simpler. Children’s needs are so overwhelming, and their dependence on us so absolute, that it’s impossible to misread our moral obligation to them. We bind ourselves to those who need us most, and through caring for them, grow to love them, grow to delight in them, grow to marvel at who they are.”
Talk About Meditation...Without Being Annoying
Mindfulness is not simply sitting still in a chair with your eyes closed, nor is it necessarily connected with religion, although all sacred traditions are associated with the value of contemplative life, periods of silence, and centering prayer. Mindfulness is an experience, not a theory or an idea or concept. Mindfulness happens within ourselves, within the mind or—as some would say—within the spirit. Whatever we choose to call the experience, or however we define it, science clearly shows the benefit of mindfulness practices.

In his book Mindful Work, David Gelles (New York Times reporter) makes a good case for mindfulness: "One of the most surprising and promising trends in business today is the rise of mindfulness in the workplace. At first, the notion of yoga and meditation in the office seems like the province of Silicon Valley startups where employees bring their dogs to work and play football in the lobby. But in recent years, mindfulness has gone mainstream. Many of America’s largest companies, such as General Mills, Target, Google, and Aetna, have built extensive programs to foster mindful practices among their workers. This is because—as employees and employers are discovering, and psychologists and cognitive scientists have confirmed—mindfulness has tangible benefits. For workers, meditation lowers stress, increases mental focus, and alleviates depression. For companies, a more mindful workforce is more productive."
1. Don’t foist it on anyone
Nobody loves a noodge who is intent on telling you what’s wrong with you and what you have to do to fix it. While you may feel that someone who is telling you how stressed out they are would benefit from meditation, it’s better to bide your time and let them ask you about it. Resist the urge to gush about your new favorite thing.
An exception: There’s nothing wrong with suggesting it to your employer. It’s not as awkward to bring it up in an organizational context. You’re not really imposing on anyone. You can talk about the science, about how lots of successful organizations are using it (See David Gelles’ Mindful Work), and suggest someone to contact. If possible, it’s good to note that any successful mindfulness program must be voluntary.
2. It’s not about stopping thinking or clearing the mind
Lots of people have picked up the truly crazy idea that meditation somehow vacuums out your head and makes you into a brainless zombie. Let people know that it’s about focusing the mind, not blanking it out. Emphasize that it’s an inherent, innate ability, a skill, not a gauzy, zoned-out place to drift off to.
3. It’s not just another damn thing on a to-do list to not do
People are naturally afraid to take on yet another self-improvement project to feel guilty about. Their life probably has a few exercise machines they’re not using, books they’re not reading, and club memberships going unused. Let them know that there are lots of ways to fit meditation into their existing life, and that it might actually help them use time better.
4. Let them know it’s hard, but not too hard
There’s no point in blathering on about how simple and easy it is, because if someone tries it for even five minutes, one of their first thoughts will be, “I cannot do this.” Staying with your breath in the moment can just seem impossible. Let people know this, but let them know it does get better.
5. If you can tell someone is interested, find out why, and listen
There’s a great New Yorker cartoon where a woman tells her lunch companion, “I’ve only been gluten-free for a week, but I’m already really annoying.” The essence of proselytizing and preaching is talking at, not with, someone. It’s important to hear what someone has to say and be ready to learn. It also sends the authentic message that mindfulness is about being continually curious about the mind—your own and everyone else’s.
6. Remind them about what really is annoying: the ceaseless voice in your head
When you talk about the nattering voice in the head, you get right into the heart of people’s internal lives, which they may or may not have considered before. If you point out that most of our internal dialogue is negative and self-referential, most people will recognize that in themselves. The notion of having a tool to better manage that will seem appealing.
7. Stick with what you know and be honest
What could hurt about telling someone here’s what I’ve done and what it’s done for me. It makes no promises and it allows you to have a real human discussion at eye level, rather than elevate yourself onto the pedestal of “great and learned meditator.”
New Video: Why Doctors Hate Electronic Medical Records
I'm not a fan of hip-hop or rap music, but I love this video. If you're not a health professional you may not understand the jargon, but the lyrics are just simply 100% reflective of the way doctors feel. Here are the lyrics, if you don't have three minutes to view the video and hear the song:
Yeah I’m out that paper, no more chasing med records
Writing so illegible, that I’ll be HIPAA foreva
Bought the new software, and though we use it here
I can’t use it over there, different systems everywhere
I used to chart on paper, all of my verbals recorded
Mix up with the ward clerk, turned “diluted” to “dilaudid”
Switched me to that EMR, meaningless abuse, G
Now catch me at the nurses station mashin’ that F2 key
Notes used to be our story, narrative, but yo
Replaced with copy paste, now a bloated ransom note
Me, I’m at that bedside, focused like a laser beam
On the patient, naw come on, I’m treatin’ the computer screen
8 dozen warnings, click check boxes
Alarm fatigue, vaseline conflicts with doxy??
Nurses they be burned out, we could use some OT
Tell by our wrist guards that we most definitely on
EHR, crappy software some vendor made us,
there’s nothing you can do, stuck with EHR,
best practice pop ups will tire you,
complain and they’ll fire you,
we need a new chart new chart new chart
(you’re welcome, they built you a turd doc!)
Catch me on the phone with IT beggin’ tech support
Shoot, it’s like IT and me be stuck in 1994
Innovation all around, but it ain’t in healthcare
Internet and apps for you, but we get ancient software
Welcome to that EHR, Go Live and it don’t stop
Uncle Sam promoted it, but gone is the interop
CMS, EMS, PMS, holla back
For doctors it ain’t fair, these vendors act like they all kinda wack
8 million stories, out there docs can’t take it,
after this disaster half of y’all won’t make it
How to train your Dragon: “hotmail” isn’t “Hot Male”
If some be saying it’s epic we sayin’ it’s epic fail
Electronic silo, team not talking
Paperless they say, but whole trees we droppin’
Props to case management
Long live the RT
Long live the pharmacist, whole team definitely hates
EHR, just a glorified billing platform,
with some patient stuff tacked on,
give us a new chart, ICD-10’s a disaster,
meet your new robot master,
we need a new chart, new chart, new chart
(this chart wack, welcome to the apocalypse doc)
Tech should bind us, connect, not blind us,
to the reason why we care,
Patient’s face reminds us
Designs like Epocrates, that tap the app agilely
Then magically the team works, let’s bite the Apple, Steve
Caught up in the in-box, now you’re in-sane
Good docs gone mad, the clinic’s filled with them
Nursing, they the heart of everything
Data entry got ‘em hurtin’, life starts when the shift ends
10 years of school, graduated to the OR
Mommy busts a Whipple she deserves a better damn chart
Autocorrect turning Chantix into Champion
Patient needs a sleeper, 30 clicks for a Ambien
EHR, crappy software some vendor made us,
there’s something you CAN do,
give us a new chart,
stand up and make our voices heard,
let doctors be doctors,
we need a new chart new chart new chart
(Stand up, the whole team)
Never Underestimate the Power of a Single Intervention
A few minutes of counseling in a primary care setting could go a long way toward steering people away from risky drug use -- and possibly full-fledged addiction, a UCLA-led study suggests. (Primary care refers to family physicians and other non-psychiatrists who provide most of our medical care.)
People who participated in the Quit Using Drugs Intervention Trial, or Project QUIT, which was a randomized controlled trial conducted in medical clinics, reduced their risky drug use by one-third when primary care doctors and health coaches provided them with brief interventions during a routine visit and follow-up phone calls.
Risky drug use is defined as the casual, frequent or binge use of illicit drugs such as cocaine, heroin and methamphetamine, or the misuse of prescription medications, without showing physiological or psychological signs of addiction. There are an estimated 68 million such drug users in the United States. These people are at risk not only for becoming addicts, but suffering attendant physical, mental health and social problems.
The study, published today in the peer-reviewed journal Addiction, is the first to demonstrate that a brief intervention led by a primary care physician can significantly reduce risky drug use among patients.
We Don't Plan to Become Addicts or Alcoholics
Most of the patients I (Dr. Talmadge) see in practice did not plan to become addicted to drugs. Casual use introduces powerful chemicals in the brain, and many of us then have our brains hijacked by these chemicals. As described in the HBO special on addictions, the human brain is an extraordinarily complex and fine-tuned communications network containing billions of specialized cells (neurons) that give origin to our thoughts, emotions, perceptions and drives. Often, a drug is taken the first time by choice to feel pleasure or to relieve depression or stress. But this notion of choice is short-lived. Why? Because repeated drug use disrupts well-balanced systems in the human brain in ways that persist, eventually replacing a person's normal needs and desires with a one-track mission to seek and use drugs. At this point, normal desires and motives will have a hard time competing with the desire to take a drug.
How Does the Brain Become Addicted?
As described in the HBO documentary, typically it happens like this:
-A person takes a drug of abuse, be it marijuana or cocaine or even alcohol, activating the same brain circuits as do behaviors linked to survival, such as eating, bonding and sex. The drug causes a surge in levels of a brain chemical called dopamine, which results in feelings of pleasure. The brain remembers this pleasure and wants it repeated.
-Just as food is linked to survival in day-to-day living, drugs begin to take on the same significance for the addict. The need to obtain and take drugs becomes more important than any other need, including truly vital behaviors like eating. The addict no longer seeks the drug for pleasure, but for relieving distress.
-Eventually, the drive to seek and use the drug is all that matters, despite devastating consequences.
-Finally, control and choice and everything that once held value in a person's life, such as family, job and community, are lost to the disease of addiction.
What brain changes are responsible for such a dramatic shift?
Research on addiction is helping us find out just how drugs change the way the brain works. These changes include the following:
Reduced dopamine activity. We depend on our brain's ability to release dopamine in order to experience pleasure and to motivate our responses to the natural rewards of everyday life, such as the sight or smell of food. Drugs produce very large and rapid dopamine surges and the brain responds by reducing normal dopamine activity. Eventually, the disrupted dopamine system renders the addict incapable of feeling any pleasure even from the drugs they seek to feed their addiction.
Altered brain regions that control decisionmaking and judgment. Drugs of abuse affect the regions of the brain that help us control our desires and emotions. The resulting lack of control leads addicted people to compulsively pursue drugs, even when the drugs have lost their power to reward.
The disease of addiction can develop in people despite their best intentions or strength of character. Drug addiction is insidious because it affects the very brain areas that people need to "think straight," apply good judgment and make good decisions for their lives. No one wants to grow up to be a drug addict, after all.
The addiction study cited above has some limitations. The results are based on participants' self-reporting, so the study may suffer from reporting bias. However, researchers found that based on urine testing, under-reporting of drug use was low. Additional limitations: not everyone in the clinic waiting rooms agreed to participate, which could impact the study's generalizability; there was some attrition during the study, though the 75 percent participation rate at follow-up compares to other studies of low income patients and drug use; and the three month follow up was relatively short.
There is a need for larger trials to gauge the QUIT program's effectiveness, but based on these findings the project appears to have the potential to fill an important gap in care for patients who use drugs, particularly in low-income communities, Gelberg said.
Read the entire report and article by clicking here.
Adderall Time in Texas
Here at the office, where I answer my own phone (and do my best to return all calls myself) I receive 4-5 calls weekly from individuals looking for a doctor who will prescribe Adderall or its long-acting cousin, Vyvanse (Lisdexamfetamine). Curious as it seems, many callers say that they are new to Dallas and need a new doctor to prescribe the medication. I say this is curious for two reasons. First, let's say that a doctor outside of Texas has a patient who is moving to Texas. One thing that prescribing doctor should do is help his or her patient to refer the individual to a reliable doctor in the new city; and apparently, many doctors from other states don't do this. Second, people taking stimulants don't usually have serious withdrawal problems, but coming off stimulants like Adderall can pose problems, because the person's brain has to adjust rapidly to the absence of the drug. The person who depends on Adderall will probably feel lethargic and "flat" when they don't have the medication on board. Students often panic, fearing they won't be able to study or put in the long hours required for academic performance.
As with other potentially risky medications (like Xanax, hydrocodone, oxycodone, etc.), the prescribing physician assumes certain risks and responsibilities in writing the prescription. I worry about this. Many patients tell me that they have only seen the doctor 3-4 times a year, and some say that they don't even see a doctor, because a mid-level practitioner (usually a nurse practitioner) writes the prescriptions under the "supervision" of a medical doctor. The typical "med check" or brief visit to renew a prescription lasts less than 20 minutes. This is not necessarily bad or wrong, but we certainly have to wonder whether the responsible doctor really knows very much about the patient. The Texas Medical Association has noted that authorities are cracking down on "pill mill" physicians in pain management clinics, and it's very likely that doctors prescribing other Schedule II ("dangerous") drugs will face similar scrutiny.
My expert opinion is that medications are very helpful in the treatment of attention deficit disorder. My further opinion is that many people, particularly students and younger adults, are using these medications inappropriately. This is one reason that I answer my own phone. I hate it when someone shows up expecting me to write controlled substances without any discussion. Yes, these are good medications that really help many people. And no, I won't write a Schedule II medication unless there's compelling clinical evidence that justifies the prescription.
Update 10/17/15: I have been reading commentaries by Larry Diller, M.D., a developmental pediatrician who has written extensively about stimulants. He has strong and generally well-informed opinions about the use and misuse of medications like Adderall, Vyvanse, Ritalin, and Concerta. His website and his opinions can be found here.
Spiritual Reflection, Contemplation
9/22 Woke up feeling pretty good for an old man. 24 Hour book was on coffee table when I sat down with my cup of java. What I got from the reading was that "each day is an opportunity to serve God." This is curiously one of those insights that often makes me smile. I call these my "baloney sandwich" moments. In 1986 I was alone in my kitchen, having just turned 40, and I was spreading mayonnaise on a slice of bread, grabbing a quick bite before charging off to whatever I had to face that day.
For reasons I have never understood, the thought occurred to me that all God asks is that we love God and serve God by doing what He would have us do. Within two seconds the experience had passed, and I was standing there with bread and baloney. How strange to think now, thirty years later, that I have never forgotten a baloney sandwich. Perhaps God was telling me that on the one hand I have "bread for the journey," and on the other hand there is "the baloney of my life." This never fails to bring a smile, because I usually expect that God should bring me a burning bush, a blinding flash of light, or at the very least the power to part the Red Sea or raise Lazarus from the dead. "No, John," God seems to say, "you're confusing the bread with the baloney. Just eat your sandwich, and I will tend the universe around you."
When Brother Lawrence wrote his letters about the Practice of the Presence of God, he said that he realized that he could feel close to God in the privacy and relative darkness of his monastic cell, but that he experienced God most clearly when he was amidst the noise, heat, and commotion in the monastery kitchen, where he had once despised his job as a distraction and a burden. Today I will think on these things as I toil and sweat, perhaps enjoying the discernment that helps me distinguish the bread from the baloney. I am smiling as I write this.
Addendum: Brother Lawrence was a man of humble beginnings who discovered a secret about living spiritual life here on earth. That "secret" is the art of "practicing the presence of God in one single act that does not end." He often stated that it is God who paints Himself in the depths of our soul. We must merely open our hearts to receive Him and His loving presence. For nearly 300 years this unparalleled classic has given both blessing and instruction to those who can be content with nothing less than knowing God in all His majesty and feeling His loving presence throughout each simple day. You can browse a copy of the book on Amazon here.
Twenty-Four Hours A Day is available through major booksellers, and also from Hazelden. Written by Richmond Walker, it's a book that offers daily thoughts, meditations and prayers to help recovering alcoholics live a clean and sober life. It is often referred to as "the little black book." The three most published A.A. authors are Bill W., Richmond Walker, and Ralph Pfau, in that order. Ralph, who lived in Indianapolis, became in 1943 the first Roman Catholic priest to get sober in A.A., and under the pen name "Father John Doe," wrote the fourteen Golden Books© along with three other books, all of them still in print and read by A.A. people today. Richmond Walker got sober in Boston in May 1942, and later moved down to Daytona Beach in Florida, where in 1948 he published Twenty-Four Hours a Day©, which became the great meditational book of early A.A. from that point on.
Job Burnout: The Basics
Ask yourself the following questions:
• Have you become cynical or critical at work?
• Do you drag yourself to work and have trouble getting started once you arrive?
• Have you become irritable or impatient with co-workers, customers or clients?
• Do you lack the energy to be consistently productive?
• Do you lack satisfaction from your achievements?
• Do you feel disillusioned about your job?
• Are you using food, drugs or alcohol to feel better or to simply not feel?
• Have your sleep habits or appetite changed?
• Are you troubled by unexplained headaches, backaches or other physical complaints?
If you answered yes to any of these questions, you may be experiencing job burnout. Be sure to consult your doctor or a mental health provider, however. Some of these symptoms can also indicate certain health conditions, such as a thyroid disorder or depression. Several times a year I encounter a patient suffering from low thyroid, iron deficiency anemia, Vitamin D deficiency, and other conditions that contribute to fatigue and burnout.
Discover if you're at risk of job burnout — and what you can do
when your job begins to affect your health and happiness.
Job burnout can result from various factors, including:
• Lack of control. An inability to influence decisions that affect your job — such as your schedule, assignments or workload — could lead to job burnout. So could a lack of the resources you need to do your work.
• Unclear job expectations. If you're unclear about the degree of authority you have or what your supervisor or others expect from you, you're not likely to feel comfortable at work.
• Dysfunctional workplace dynamics. Perhaps you work with an office bully, you feel undermined by colleagues or your boss micromanages your work. These and related situations can contribute to job stress.
• Mismatch in values. If your values differ from the way your employer does business or handles grievances, the mismatch may eventually take a toll.
• Poor job fit. If your job doesn't fit your interests and skills, it may become increasingly stressful over time.
• Extremes of activity. When a job is always monotonous or chaotic, you need constant energy to remain focused — which can lead to fatigue and job burnout.
• Lack of social support. If you feel isolated at work and in your personal life, you may feel more stressed.
• Work-life imbalance. If your work takes up so much of your time and effort that you don't have the energy to spend time with your family and friends, you may burn out quickly.
You may be more likely to experience job burnout if:
• You identify so strongly with work that you lack a reasonable balance between your work life and your personal life
• You try to be everything to everyone
• You work in a helping profession, such as health care, counseling or teaching
• You feel you have little or no control over your work
• Your job is monotonous
Ignored or unaddressed job burnout can have significant consequences, including:
• Excessive stress
• Fatigue
• Insomnia
• A negative spillover into personal relationships or home life
• Depression
• Anxiety
• Alcohol or substance abuse
• Heart disease
• High cholesterol
• Type 2 diabetes, especially in women
• Stroke
• Obesity
• Vulnerability to illnesses
Don't let a demanding or overwhelming job undermine your health.
Remember, if you think you may be experiencing job burnout, don't ignore your symptoms. Consult your doctor or a mental health provider to identify or rule out any underlying health conditions.If you're concerned about job burnout, take action. To get started:
- Manage the stressors that contribute to job burnout. Once you've identified what's fueling your feelings of job burnout, you can make a plan to address the issues.
- Evaluate your options. Discuss specific concerns with your supervisor. Perhaps you can work together to change expectations or reach compromises or solutions. Is job sharing an option? What about telecommuting or flexing your time? Would it help to establish a mentoring relationship? What are the options for continuing education or professional development?
- Adjust your attitude. If you've become cynical at work, consider ways to improve your outlook. Rediscover enjoyable aspects of your work. Recognize co-workers for valuable contributions or a job well done. Take short breaks throughout the day. Spend time away from work doing things you enjoy.
- Seek support. Whether you reach out to co-workers, friends, loved ones or others, support and collaboration may help you cope with job stress and feelings of burnout. If you have access to an employee assistance program (EAP), take advantage of the available services.
- Assess your interests, skills and passions. An honest assessment can help you decide whether you should consider an alternative job, such as one that's less demanding or one that better matches your interests or core values.
- Get some exercise. Regular physical activity, like walking or biking, can help you to better deal with stress. It can also help get your mind off work and focus on something else.
- Pay attention to your use of alcohol, pills, or other "stress relievers." Although booze and drugs can provide temporary relief, neuroscience tells us that the misuse of alcohol or intoxicants is bad for your brain. It's better to get proper help from a qualified professional.
60 Minutes: Managed Care & Mental Health
CBS and 60 Minutes produced a chilling and dramatic segment on mental health and managed care.
Three years ago, we were reeling from the shock of the murders of 20 first graders and six educators at Sandy Hook Elementary School. Since then, we've learned that the killer suffered profound mental illness. His parents sought treatment but, at least once, their health insurance provider denied payment.
Because of recurring tragedies and an epidemic of suicides, 60 Minutes investigated the battles that parents fight for psychiatric care. CBS found that the vast majority of claims are routine but the insurance industry aggressively reviews the cost of chronic cases. Long-term care is often denied by insurance company doctors who never see the patient. As a result, some seriously ill patients are discharged from hospitals over the objections of psychiatrists who warn that someone may die.
An article in one of the academic journals, Administration Policy and Mental Health, states: "A diverse array of managed care techniques have been introduced into the profession of psychiatry in an effort to alter treatment patterns. One commonly used tool, utilization review, can alter treatment patterns by restricting access to treatment alternatives and providing incentives to practitioners to meet managed care goals. Other managed care tools are the determination of "medical necessity" and the use of triage and treatment guidelines among insured enrollees requesting services. These guidelines serve as selection criteria to help determine not only which members of the insured population receive treatment for mental health care, but also to determine the allocation of enrollees to staff members and to prescribe the starting point for the types of services received. Managed care psychiatrists may find changes not only in their client populations and treatment alternatives, but in many other aspects of their practice."
The 60 Minutes segment focuses on Anthem, an insurance company said to have a 90% denial rate. One of the many lawsuits filed against Anthem is detailed here. Many consumer complaints about Anthem are listed here.
To see this dramatic report from 60 Minutes and CBS News, click here.
Back from Vacation...
Not taking vacation time is a bad idea, as it harms productivity and the economy. Those are key findings of a new study released earlier this month.
More than forty percent of American workers who received paid time off did not take all of their allotted time last year, despite the obvious personal benefits, according to “An Assessment of Paid Time Off in the U.S.” commissioned by the U.S. Travel Association, a trade group, and completed by Oxford Economics.
Americans left an average of 3.2 paid time off days unused in 2013, totaling 429 million unused days for U.S. workers.
According to the study, most managers recognize the benefits taking time off from work provide to employees: higher productivity, stronger workplace morale, greater employee retention, and significant health benefits. But nearly 34 percent of employees surveyed indicated that their employer neither encouraged nor discouraged leave, and 17 percent of managers considered employees who take all of their leave to be less dedicated, according to the survey’s findings.
And four in ten American workers said their employer supported time off, but their heavy workload kept them from using their earned days.
“Despite the myriad benefits of taking time off, American workers succumb to various pressures-some self-imposed and some from management-to not take the time off to which they are entitled,” Adam Sacks, president of the Tourism Economics division of Oxford Economics, said in a statement. “Leaving earned days on the table harms, not helps, employers by creating a less productive and less loyal employee.
“Further, it is a misconception that employers are ahead of the game when workers don’t use the time they’ve earned,” he added. “In fact, stockpiled time off creates considerable financial liability for companies and governments when employees ‘cash out’ upon departure.”
The primary research for the study was based on an online survey conducted between September and October 2013. The sample included 971 employees, 700 of whom receive paid time off as part of their benefits package.
Mindfulness and PTSD
Mindfulness is the intentional, accepting and non-judgemental focus of one's attention on the emotions, thoughts and sensations occurring in the present moment, which can be trained by meditational practices. Although linked to Buddhism and eastern philosophies, many Christians practice mindfulness. It is not a religious practice, nor is it tied to a specific set of religious beliefs. An excellent article on Christianity and mindfulness by Dr. Scott Symington can be found in the Journal of Psychology and Christianity if you click here.
Many psychiatrists and psychologists have moved away from the labels of psychiatry—bearing in mind that diagnosis and traditional treatment are often very helpful—to incorporate mindfulness based practices in our work. Dr. Melissa Polusny from the Minneapolis VA Health Care System, and colleagues randomly assigned 116 veterans with PTSD to nine sessions of either mindfulness-based stress-reduction (MBSR) therapy or present-centered group therapy, which focused on current life problems.
Dr. Ellis-Jones comments on his blog: "The researchers found that during treatment and in the two months following, MBSR therapy improved PTSD symptoms more than did present-centered group therapy. In fact, those who had MBSR experienced a 49 per cent reduction in PTSD symptoms, compared with a 28 per cent reduction in symptoms among those who had present-centered group therapy."
News Flash! Interesting Articles...
Should a Worker Be Fired for Using Medical Marijuana at Home? Healthline , By R. Sam Barclay, July 9, 2015 Advocates Push to Expand Use of Medications to Treat Addiction USA Today , By Liz Szabo, July 8, 2015 Virtual Reality Shows How Dangerous it is to Drive Drunk and Stoned PBS NewsHour , By Catherine Woods, June 27, 2015 Neuroscience: Rewiring the Brain Nature , By Katherine Bourzac, June 25, 2015 Genetics: No More Addictive Personality Nature , By Maia Szalavitz, June 24, 2015 "Pharmacotherapy: Quest for the Quitting Pill" Nature , By Cassandra Willyard, June 24, 2015 Study Analyzes How Much Pot Impairs Drivers USA Today , By Trevor Hughes, June 23, 2015 "How Much Does Marijuana Impact Your Driving?" TIME , By Eliza Gray, June 23, 2015 "Designer Drugs Hit Dangerous Lows to Bring New Highs" Science News , By Kate Baggaley, May 05, 2015
Stages of Change: A Summary
Stages of Change
The Stages of Change, as described in the treatment of alcoholism and other addictions, can be summarized in five parts. The stages are best conceptualized as a cycle. Alcoholics and addicts cycle through the stages, sometimes three or four times, before they complete the cycle without a slip or a relapse. This can be very frustrating for all concerned. But that's the nature of the game.
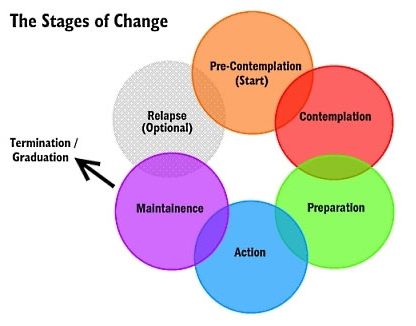
1) PRECONTEMPLATION STAGE
"It isn't that we can't see the solution. It's that we can't even see the problem for what it is."
Pre-contemplators usually show up in therapy because of pressures from others: spouses, employers, parents, and courts. They resist change. When their problem comes up, they change the topic of conversation. They place responsibility for their problems on factors such as genetic makeup, addition, family, society, destiny, the police. They explain how little they actually use or drink, and they complain that no one gives them credit when they cut down or even abstain for a short time. They feel hopeless and demoralized, and they are often defensive, angry, and frankly illogical in their thinking.
2) CONTEMPLATION STAGE
"I want to stop feeling so stuck. I am tired of all the hassles and of other people intruding in my life."
Contemplators admit that they have a problem and begin to think about solutions. Contemplators struggle to understand their problems, to see its causes, and wonder about possible solutions. Many contemplators have indefinite plans to take action within the next few months. They know where they want to do, and they have ideas (some good, some not so good) about how to get there.
"You know your destination, and maybe even how to get there, but you're not ready to go…yet."
Contemplators tell themselves that someday they are going to change. When contemplators are trying to reach the preparation stage of change, their thinking is clearly marked by two changes.
First, they begin to think more about the future than the past.
The end of contemplation stage is a time of anticipation and anxiety. Relapse is common when individuals reach this stage. They are fearful of what will happen next. Support from family and friends may be exhausted. Even though they have made considerable effort, things often don't get easier — not yet.
Between stage 2 and 3: A decision is made. People conclude that the negatives of their behavior outweigh the positives. They choose to change their behavior. They make a commitment to change. This decision represents an event, not a process.
3) PREPARATION STAGE
Most people in the preparation stage are planning to take action and are making the final adjustments before they begin to change their behavior. Usually they have not resolved their ambivalence. A part of them wants to get well, but as the Zen saying puts it, "The mind is a barrel of wild monkeys," and they often go back and forth about taking action.
4) ACTION STAGE
The time for action does not come on with a blinding flash of light. There is no burning bush. Gradually the person overtly modifies his or her behavior and his or her surroundings. At this point the make the move for which they have been preparing. This is a critical point, and it requires the greatest commitment of time and energy.
Change is visible to others. Others can see the difference in attitude, honesty and commitment. Small changes sometimes matter the most.
5) MAINTENANCE STAGE
Change never ends with a single action. One old saying in Alcoholics Anonymous is that without a strong commitment to maintenance, there will surely be relapse, usually to the pre-contemplation or contemplation stage.
THE IMPORTANCE OF PROCESSES
Processes are selected activities that are regularly initiated to effect change. There are nine important ones chosen by therapists as distinct areas of consideration and useful tools in personal transformation.
1. Consciousness-raising: Increasing knowledge about yourself and your problem.
2. Social liberation: Considerations in the external environment that can contribute to helping change, i.e.: no smoking areas, lo-cal menu items, advocacy groups.
3. Emotional arousal: Increased awareness through depth of feeling from natural events or dramatic intervention, psychodrama.
4, Self-reevaluation: A thoughtful and emotional reappraisal of yourself as regards your problem, weighing the pros and cons of changing.
5. Commitment: Acknowledging that you are the only one who can respond, speak and act for yourself.
6. Countering: Planning for and substituting healthy responses for unhealthy ones, action oriented.
7. Environmental control: Restructuring your personal environment so that the probability of a problem-causing event is reduced.
8. Rewards: Affirmation of desirable behavior by self or others as contrasted with and better than any type of punishment for problem behavior.
9. Helping relationships: Receiving care, support and assistance from significant people in your life.
For more information about the stages of change, see the book Changing for Good by James Prochaska.
Mindfulness Therapy: Alternative to Antidepressants
Mindfulness-based cognitive therapy aims to change the way people think and feel about their experiences. How we think affects how we feel. And the use of mindfulness practice is relatively easy for most people. Just 10-15 minutes two or three times daily makes a difference. The current study compares MBCT with maintenance antidepressant medication for reducing the risk of relapse in depression. The results are encouraging.
The study aimed to establish whether MBCT is superior to maintenance antidepressant treatment in terms of preventing relapse of depression. Although the findings show that MBCT isn't always more effective than maintenance antidepressant treatment in preventing relapse of depression, the results, combined with those of previous trials, suggest that MCBT may offer similar protection against relapse or recurrence for people who have experienced multiple episodes of depression, with no significant difference in cost.
"Mindfulness gives me a set of skills which I use to keep well in the long term. Rather than relying on the continuing use of antidepressants mindfulness puts me in charge, allowing me to take control of my own future, to spot when I am at risk and to make the changes I need to stay well." — Study Participant
MBCT builds on the insight that when people with a history of depression experience even a brief period of feeling low they tend to be especially vulnerable to negative thinking. That negative thinking is often accompanied by what’s known as “processing biases”: worrying about past problems, for example, or returning to unpleasant memories. Thinking like this raises the risk of a full-blown depressive episode.
MBCT focuses on helping people to become more aware of these thoughts and feelings, and thus better able to gain distance from them. As its founders put it: “We discover that difficult and unwanted thoughts and feelings can be held in awareness, and seen from an altogether different perspective – a perspective that brings with it a sense of warmth and compassion to the suffering we are experiencing.”
Talk Therapy? Medication?
I am an old-timer, and when my generation trained in psychiatry virtually all of us planned on being psychotherapists who were well educated in the use of medication as an adjunct to talk therapy. All psychiatrists I knew back then had been in psychotherapy themselves; personal therapy was considered part of becoming a competent clinician: "Physician, know thyself."
If a psychiatrist has a limited vocabulary, and can't conjugate nouns and verbs, how can they possibly communicate with patients?
Research shows that when psychotherapy and medication are both available, the combination is synergistic. It's like saying 1 + 1 = 3. Today, however, fewer than 10% of psychiatrists are trained and skilled in psychotherapy. My opinion is that this is why a good psychiatrist is very hard to find. I have been teaching young psychiatrists for over thirty years, and I have been a training director in one of our finest medical schools, and I can say with authority that many psychiatrists coming out today get failing grades when it comes to important skills like writing, speaking, and communicating clearly. I'm talking about basic errors in English grammar, syntax, and sentence structure — the stuff most people should learn by the time they enter high school! If a psychiatrist has a limited vocabulary, and can't conjugate nouns and verbs, how can they possibly communicate with patients? This is one reason that psychiatrists today are, in general, poor psychotherapists with little interest in what talk therapy has to offer.
Writing in a medical chart is similar to text messaging. It's easy, and grammar doesn't count. In fact, the modern electronic medical record discourages thoughtful writing, just like text messaging does. A good psychiatrist should not only speak well and write well. A good psychiatrist should be a superior thinker and communicator. Every doctor should have a big sign on the wall behind the chair where the patient is sitting: "DOCTOR, YOUR PATIENT IS TRYING TO TELL YOU SOMETHING!"
Here's Dr. Friedman again: "With few exceptions, every major class of current psychotropic drugs — antidepressants, antipsychotics, anti-anxiety medications — basically targets the same receptors and neurotransmitters in the brain as did their precursors, which were developed in the 1950s and 1960s."
"Sure, the newer drugs are generally safer and more tolerable than the older ones, but they are no more effective."
Prescribing a pill is easier and cheaper than offering the patient psychotherapy. Psychiatrists are paid more to prescribe pills than to counsel with patients. It is understandable, then, that the incentive is to see five patients in a single clinic hour. This saves insurance companies a lot of money. Many insurance companies will not even pay for psychotherapy with a qualified psychiatrist. And think about this: if a patient doesn't like the psychiatrist, there are fewer repeat or return visits. The winners are the insurance companies.
Dr. Friedman is also critical of trends in research, not because they are wrong, but because of simplistic logic. "The doubling down on basic neuroscience research" he says, "seems to reflect the premise that if we can unravel the function of the brain, we will have a definitive understanding of the mind and the causes of major psychiatric disorders." He points to an editorial in May in one of the most respected journals in our field, JAMA Psychiatry, emphasizing the brain but not mentioning the mind, the complexity of mental illness, or anything about how psychotherapy scientifically helps the brain. Friedman believes that "an undertaking as ambitious as unraveling the function of the brain would most likely take many years. Moreover, a complete understanding of neurobiology is unlikely to elucidate the complex interactions between genes and the environment that lie at the heart of many mental disorders."
"Anyone who thinks otherwise should remember the Decade of the Brain, which ended 15 years ago without yielding a significant clue about the underlying causes of psychiatric illnesses."
—Professor and Psychiatrist Richard Friedman
Dr. Friedman's article generated a number of replies, including this one from Christopher Lukas, a noted author:
"Over the years, I have had talking therapy for my depression and post-traumatic stress disorder, and I don’t believe I would be alive were it not for those sessions. I have also taken a whole range of medications for depression and find that psychotherapy outweighs the benefits of any of those drugs.
"Some psychiatrists and some patients think that drugs are better because they work like aspirin: Take two and call me in the morning. But, as Dr. Friedman pointed out, and as I have experienced, other patients find doses of talking therapy can work well if we’re patient and if we understand that many emotional problems may take time to go away.
"Persistence, willingness to give yourself over to the process and willingness to change therapists if the talk isn’t helping you: These are key to talk therapy’s benefits."
The comments by Lukas remind me of something I pointed out to a patient just last weekend. Asking about Alcoholics Anonymous, she wanted to know what it takes to succeed in finding sobriety through AA. "An easy way to think about it," I said, is to remember the three letters H-O-W." The old AA acronym stands for "honesty, open-mindedness, and willingness."
Another writer, who is a physician herself, also agreed with Dr. Friedman:
"For the past 30 years psychotherapy has been given short shrift as drug therapy has become the treatment of choice. There are many reasons for this, but the most powerful are economic.
"Doctors can manage medication for many more patients in a day than they can treat with psychotherapy. More important, pharmaceutical companies, which profit from the drug sales, support research, thus providing funds to psychiatry departments that receive no similar support for psychotherapy research. Sadly, in the past generation or two there has been a huge loss in professional expertise as fewer psychiatry residency programs provide top-notch psychotherapy education and supervision.
"Twenty-eight years ago I went to medical school planning a career in child psychiatry. My interest had been primed by fascinating conversations I’d heard in high school between my father, a psychoanalyst, and his colleagues. My medical school psychiatry rotation was a disappointment. There was no attempt to solve the riddles of patients’ emotions and behavior, only the adjustment of medication doses to treat symptoms. Still wanting to solve puzzles, I chose a career in radiology.
"When my father died, I was tremendously moved to hear some of his patients who attended his funeral tell me how the treatment he provided had profoundly changed their lives. Psychotherapy should be an integral part of psychiatric training."
Since I do both — I am a psychotherapist who prescribes medication when appropriate — it's understandable that I agree with Dr. Friedman. It's also true that I practice this way because that approach provides the best care for the brain, the mind, and the whole person.
The Adderall Phone Call Trend
The underground trade in stimulants is massive. People will pay $20 for a single pill on the street.
ADD medications like Adderall and Ritalin are stimulants, amphetamines or amphetamine-related compounds. They can be miraculously helpful when the doctor has the right diagnosis and prescribes them appropriately. I am a big believer in the value of such medications, because they work. I also know from experience that they can be terribly abused.
Here are some tips from the American Academy of Child and Adolescent Psychiatry:
Many students with Attention Deficit Hyperactivity Disorder (ADHD) attend college. College students with ADHD face a number of challenges, including choosing a supportive school and community where they can find and access medical services, get help with organizing their schedule and life, and succeed academically
Most people with ADHD are diagnosed before college. However, some people may not recognize the signs and symptoms of ADHD until they are at college. Trying to balance school work and the freedom of living away from home for the first time may be challenging. It can be natural to feel unfocused, distracted, overwhelmed, or disorganized when attending college. However, if these issues have caused significant problems in the past and are getting in the way of current functioning, the student may have ADHD.
If a student is struggling, it may be helpful to seek consultation with a qualified mental health professional. The diagnosis of ADHD is made based on a comprehensive clinical assessment. This may include information from multiple sources, including rating scales, getting history from the student, family, or past teachers if possible. There is no single test (brain imaging, blood testing, or psychological testing) that can reliably diagnose ADHD. Research shows that medication is the most effective treatment for ADHD. Cognitive-behavioral therapy, social skills training, and academic support can also be helpful.
There are many ways to successfully manage ADHD before and during college.
Preparing for and Staying Organized While at College
Consider the best college environment to meet your needs, such as class size, workload, academic calendar, and availability of support services. Resources to help you find the best college include: high school counselors, parents, friends who are in or have attended college, and national ADHD organizations or websites.
Learn about the medical services available at colleges before choosing where to go. Some college and university health centers do not prescribe ADHD medications. You may need to find a doctor in the surrounding community. Think about the transportation options and ease of access to that provider.
Talk with your doctor about how to best manage your medications when at college. Do not make changes in your medication without consulting your doctor. Ask your current doctor and the doctor at college to coordinate care. It is also helpful to have a history of your medications and your response to those medications for your new doctor.
If you have used tutors or support before college, think about continuing at college, at least for a little while.
If you need specific support or accommodations, register at the college disability office. If you have a summary of treatment or any psychological tests that were done within the last 3 years, bring them to the visit.
Practice using planners, calendars, or scheduling apps while still in high school. The demands on time management and organization increase greatly in college. Even if your parents helped you in the past, it is important to learn to do it yourself.
Managing Medications at College
Many medications prescribed for ADHD have to be monitored regularly. While at college, you need to schedule and keep your own medical appointments. Changes to your medication should only be made after talking with your doctor.
Learn how to use pharmacy services. Pay attention to prescription start dates and expiration dates. Many medications prescribed for ADHD are “controlled substances” so states may have additional rules on how these medicines can be provided, including limits on how often prescriptions can be refilled.
Taking medication that is not prescribed for you, sometimes called “diversion” or “academic doping,” is illegal and unsafe. Your medications were prescribed by your doctor who knows you and your medical history. They should only be taken by you. There are serious cardiac, neurological, and psychological risks of misusing ADHD medications. There can also be serious risks to mixing medications with alcohol or other drugs.
Keep medications safely stored or hidden to protect against theft. If medications are stolen, report it to campus or local police.
Adjusting to the academic, social, and organizational demands of college is difficult for most students. It can be especially difficult for students with ADHD. Arranging for support from medical and school professionals can help students with ADHD have a successful college experience, as well as a long career after graduation.
Should Children Take Antipsychotic Drugs?
According to Scientific American: "Modern antipsychotic drugs are increasingly prescribed to children and adolescents diagnosed with a broad variety of ailments. The drugs help to alleviate symptoms in some disorders, such as schizophrenia and bipolar disorder, but in others their effectiveness is questionable. Yet off-label prescribing is on the rise, especially in children receiving public assistance and Medicaid. Psychotic disorders typically arise in adulthood and affect only a small proportion of children and adolescents. Off-label prescriptions, however, most often target aggressive and disruptive behaviors associated with attention-deficit hyperactivity disorder (ADHD). “What's really concerning now is that a lot of this prescription is occurring in the face of emerging evidence that there are significant adverse effects that may be worse in youth than in adults,” says David Rubin, a general pediatrician and co-director of PolicyLab at Children's Hospital of Philadelphia. Here we review the evidence for the effectiveness of antipsychotic medications commonly prescribed for five childhood conditions. But do the benefits outweigh the risks?" To read the entire article, click here.
The mental health system can sometimes be complicated and difficult for parents to understand. A child's emotional distress often causes disruption to both the parent's and the child's world. Parents may have difficulty being objective. They may blame themselves or worry that others such as teachers or family members will blame them.
If you are worried about your child's emotions or behavior, you can start by talking to friends, family members, your spiritual counselor, your child's school counselor, or your child's pediatrician or family physician about your concerns. If you think your child needs help, you should get as much information as possible about where to find help for your child. Parents should be cautious about using the internet as their only source of information and referral.
Whole Brain Teaching
Research on the brain and how we think and act is influencing the way some teachers teach. Special correspondent John Tulenko of Learning Matters goes into a classroom where the instructor uses different methods to engage different parts of the students’ brains, then checks with a neuroscientist about whether that strategy actually works.
Whole Brain Teachers of America is a grass roots, education reform movement begun in 1999 by three Yucaipa, California teachers: Chris Biffle (college), Jay Vanderfin (elementary school) and Chris Rekstad (elementary school).
Whole Brain Teaching rests upon the principle that teachers at every level share the same difficulties: students lack discipline, background knowledge and fundamental problem solving skills. From kindergarten to college, teachers face students who have difficulty with reading and writing. Nonetheless, our students respond to challenges, enjoy well-designed learning games, and can make, in the proper setting, astonishing educational progress.
From their website: "At the root of Whole Brain Teaching is a large amount of highly structured, educational tomfoolery. Students learn the most when they are having fun. Whole Brain Teaching classrooms are full of task-focused laughter. Humor and games are used to increase the number of times students repeat core information and practice basic skills. Classes are highly disciplined and tightly organized because students have more fun following our rules, than ignoring them."
Drug Overdose Deaths, Injuries
The good news? We are better off than 38 other states when it comes to events like drug overdose, car wrecks, killings, drownings, and the million other ways to die in The West. I just reviewed the report sponsored by the Robert Wood Johnson Foundation, a leading source of funding for medical research and education.
In The Facts Hurt: A State-By-State Injury Prevention Policy Report, Texas ranked 39th highest for the number of injury-related deaths in the state, with a rate of 55.3 per 100,000 people. Overall, the national rate is 58.4 per 100,000.
Rates in Texas decreased over the past four years for injury deaths, which includes drug overdoses, motor vehicle crashes, homicides and others. Overall, 17 states increased, 24 remained stable and 9 decreased. Injuries are the leading cause of death for Americans ages 1 to 44 – and are responsible for nearly 193,000 deaths per year.
Drug overdoses have become the leading cause of injury in 36 states, not including Texas, surpassing motor vehicle-related deaths.
Some key findings include:
Drug abuse: More than 2 million Americans misuse prescription drugs. The prescription drug epidemic is also contributing to an increase in heroin use; the number of new heroin users has doubled in the past seven years.
Key report indicators include the finding that 34 states and Washington, D.C. have “rescue drug” laws in place to expand access to, and use of naloxone - a prescription drug that can be effective in counteracting an overdose - by lay administrators. This is double the number of states with these laws in 2013 (17 and Washington, DC). While every state except Missouri has some form of Prescription Drug Monitoring Program (PDMP) in place to help reduce doctor shopping and bad prescribing, only half (25) require mandatory use by healthcare providers in at least some circumstances.
Motor vehicle deaths: Rates have declined 25 percent in the past decade (to 33,000 per year).
Key report indicators include observation that 21 states have drunk driving laws that require ignition interlocks for all offenders;
and while most states have Graduated Drivers Licenses that restrict times when teens can drive, 10 states restrict nighttime driving for teens starting at 10 pm; and 35 states and Washington, D.C. require car safety or booster seats for children up to age 8.
Homicides: Rates have dropped 42 percent in the past 20 years (to 16,000 per year).
The rate of Black male youth (ages 10 to 24) homicide victims is 10 times higher than for the overall population. One in three female homicide victims is killed by an intimate partner. Research shows that 31 states have homicide rates at or below the national goal of 5.5 per every 100,000 people.
Suicides: Rates have remained stable for the past 20 years (41,000 per year). More than one million adults attempt suicide and 17 percent of teens seriously consider suicide each year. Seventy percent of suicides deaths are among White males.
Falls: One in three Americans over the age of 64 experiences a serious fall each year, falls are the most common nonfatal injuries, and the number of fall injuries and deaths are expected to increase as the Baby Boomer cohort ages.
A key report indicator includes: 13 states have unintentional fall-related death rates under the national goal (of 7.2 per 100,000 people – unintentional falls).
Traumatic brain injuries: (TBIs) from sports/recreation among children have increased by 60 percent in the past decade.
Nationally, drug overdose deaths have more than doubled in the past 14 years – resulting in 44,000 deaths per year, and half of those deaths (22,000) are related to prescription drugs. Texas ranked sixth lowest for drug overdose deaths—at a rate of 9.6 per 100,000 people.
Texas scored three out of 10 on key indicators of steps states can take to prevent injuries – nationally, 29 states and Washington, D.C. scored a five or lower. New York received the highest score of nine out of a possible 10 points, while four states scored the lowest, Florida, Iowa, Missouri and Montana, with two out of 10 points.
Drug overdoses are the leading cause of injury deaths in the United States, at nearly 44,000 per year. Prescription drugs are the leading cause.
These deaths have more than doubled in the past 14 years, and half of them are related to prescription drugs (22,000 per year). Overdose deaths now exceed motor vehicle-related deaths in 36 states and Washington, D.C. And, in the past four years, drug overdose death rates have significantly increased in 26 states and Washington, D.C. and decreased in six.
The Facts Hurt report uses10 key indicators of leading evidence-based strategies that help reduce injuries and violence. The indicators were developed in consultation with top injury prevention experts from the Safe States Alliance and the Society for the Advancement of Violence and Injury Research (SAVIR).
The 10 indicators include:
▪ Does the state have a primary seat belt law? (34 states and Washington, D.C. meet the indicator and 16 states do not.)
▪ Does the state require mandatory ignition interlocks for all convicted drunk drivers, even first-time offenders? (21 states meet the indicator and 29 states and Washington, D.C. do not.)
▪ Does the state require car seats or booster seats for children up to at least the age of 8? (35 states and Washington, D.C. meet the indicator and 15 do not.)
▪ Does the state have Graduated Driver Licensing laws - restricting driving for teens starting at 10 pm? (11 states meet the indicator and 39 states and Washington, D.C. do not. Note a number of other states have restrictions starting at 11 pm or 12 pm.)
▪ Does the state require bicycle helmets for all children? (21 states and Washington, D.C. meet the indicator and 29 states do not.)
▪ Does the state have fewer homicides than the national goal of 5.5 per 100,000 people established by the U.S. Department of Health and Human Services (HHS) (2011-2013 data)? (31 states meet the indicator and 19 states and Washington, D.C. do not.)
▪ Does the state have a child abuse and neglect victimization rate at or below the national rate of 9.1 per 1,000 children (2013 data)? (25 states meet the indicator and 25 states and Washington, D.C. do not.)
▪ Does the state have fewer deaths from unintentional falls than the national goal of 7.2 per 100,000 people established by HHS (2011-2013 data)? (13 states meet the indicator and 37 states and Washington, D.C. do not.)
▪ Does the state require mandatory use of data from the prescription drug monitoring program by at least some healthcare providers? (25 states meet the indicator and 25 states and Washington, D.C. do not.)
▪ Does the state have laws in place to expand access to, and use of, naloxone, an overdose rescue drug by laypersons? (34 states and D.C. meet the indicator and 16 states do not.)
Score Summary: Texas Scores 3 out of 10
For the state-by-state scoring, states received one point for achieving an indicator or zero points if they did not achieve the indicator. Zero is the lowest possible overall score, 10 is the highest.
9 out of 10: New York
8 out of 10: Delaware
7 out of 10: California, New Jersey, North Carolina, Tennessee, Washington and West Virginia
6 out of 10: Alaska, Colorado, Hawaii, Indiana, Kentucky, Louisiana, Maine, Minnesota, Nevada, New Mexico, Oregon, Rhode Island and Virginia
5 out of 10: Alabama, Arkansas, Connecticut, Georgia, Illinois, Kansas, Massachusetts, Oklahoma, Utah, Vermont and Wisconsin
4 out of 10: Arizona, District of Columbia, Idaho, Maryland, Michigan, Mississippi, New Hampshire, North Dakota and Pennsylvania
3 out of 10: Nebraska, Ohio, South Carolina, South Dakota, Texas and Wyoming
2 out of 10: Florida, Iowa, Missouri and Montana
Bogus: Dr. Oz
This is an issue I have addressed before on this blog where my focus has been on quackery associated with the use of expensive neuroimaging or "brain scans" claiming to diagnose a variety of psychiatric problems like attention deficit disorder, addictions, and mood problems. Although neuroimaging is very promising, getting a scan does not change diagnosis or treatment for these kinds of disorders. One of the egregious offenders is Dr. Daniel Amen, perhaps the best known psychiatrist in America, whose self-produced PBS specials air widely on public television and promote his unproven claims about scans. Although Amen claims that his theories are based on thousands of cases, experts in the field have widely condemned his misrepresentation of the facts.
The AMA is finally taking a stand on quack doctors who spread pseudoscience in the media.
The AMA will look at creating ethical guidelines for physicians in the media, write a report on how doctors may be disciplined for violating medical ethics through their press involvement, and release a public statement denouncing the dissemination of dubious medical information through the radio, TV, newspapers, or websites.The move came out of the AMA's annual meeting in Chicago this week, where medical students and residents pushed the AMA after noticing that the organization was mostly silent during the recent public debates about the ethics of Dr. Oz sharing unfounded medical advice on his exceptionally popular TV show.
"Dr. Oz has something like 4 million viewers a day," student representatives said. "The average physician doesn't see a million patients in their lifetime. That's why organized medicine should be taking action."
Last summer, Oz was called before a Senate subcommittee on consumer protection, where the senator in charge, Claire McCaskill (D-MO), asked him to explain his use of "flowery" language to champion weight loss fixes that don't actually work and then admonished him for endorsing a rainbow of supplements as potential "belly blasters"and "mega metabolism boosters." As McCaskill put it, "The scientific community is almost monolithic against you in terms of the efficacy of the three products you called 'miracles.'"
In December, a British Medical Journal study examined the health claims showcased on 40 randomly selected episodes of the two most popular internationally syndicated health talk shows — The Dr. Oz Show and The Doctors — and found that about half of the recommendations either had no evidence behind them or actually contradicted the best available science.
In January, investigations into The Dr. Oz Show by the Federal Trade Commission showed that at least one of Oz's miracle-touting guests used the program as a platform to deceive audiences and sell products.
In April, a high-profile group of physicians and academics questioned Oz's faculty position at Columbia University and wrote in a letter to the medical school dean: "Dr. Oz is guilty of either outrageous conflicts of interest or flawed judgments about what constitutes appropriate medical treatments, or both." The same month, Oz responded to his critics by accusing them of having conflicts of interest and defending his civil liberties. "I know I have irritated some potential allies," he wrote in Time magazine. "No matter our disagreements, freedom of speech is the most fundamental right we have as Americans. We will not be silenced."
What Dr. Oz does not understand is that questions about ethics are not questions about "free speech." By his logic, a doctor can say virtually anything, make any claim, asserting that he or she has the right to freedom of speech. This is a terrible kind of logic, and it makes no sense at all.
Then again, many claims made by Dr. Oz make no sense, either.
One Nation, Under Sedation
Houston, we have a problem. For the full story, click here.
The distinguished addiction specialist Charles O'Brien, M.D., authored a paper in 2005 discussing the risks of benzodiazepine abuse. The summary of his article states: "Although benzodiazepines are invaluable in the treatment of anxiety disorders, they have some potential for abuse and may cause dependence or addiction. It is important to distinguish between addiction to and normal physical dependence on benzodiazepines. Intentional abusers of benzodiazepines usually have other substance abuse problems. Benzodiazepines are usually a secondary drug of abuse-used mainly to augment the high received from another drug or to offset the adverse effects of other drugs. Few cases of addiction arise from legitimate use of benzodiazepines. Pharmacologic dependence, a predictable and natural adaptation of a body system long accustomed to the presence of a drug, may occur in patients taking therapeutic doses of benzodiazepines. However, this dependence, which generally manifests itself in withdrawal symptoms upon the abrupt discontinuation of the medication, may be controlled and ended through dose tapering, medication switching, and/or medication augmentation. Due to the chronic nature of anxiety, long-term low-dose benzodiazepine treatment may be necessary for some patients; this continuation of treatment should not be considered abuse or addiction."
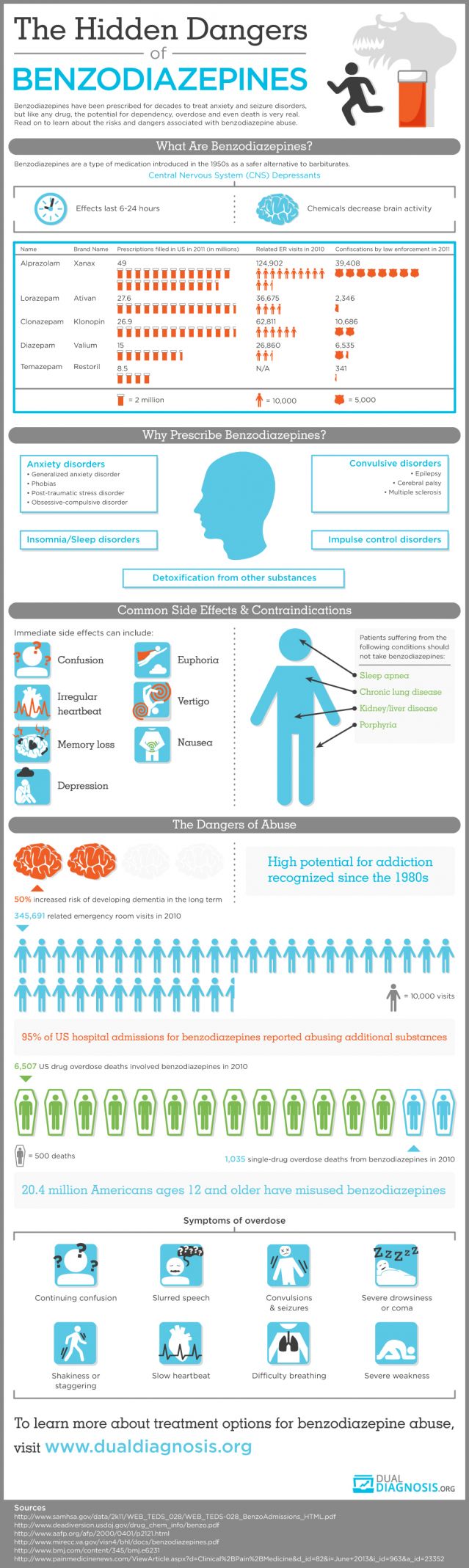
Female Veteran Suicides
Women are generally a lot less likely to kill themselves than men, but female veterans are an exception with shockingly high suicide rates, according to new Veterans Affairs Department research. Among women of all ages who have served in the military, the suicide rate is 28.7 per 100,000—higher than the rate among male civilians, nearly six times the rate of civilian women, and approaching the 32.1 rate among male veterans. "It's staggering," a Northeastern University epidemiologist said to the Los Angeles Times. "We have to come to grips with why the rates are so obscenely high." Women vets ages 18 to 29 kill themselves at nearly 12 times the rate of civilian women the same age, but the rate was up to eight times higher even among women who served in the 1950s. It is not clear what is driving the rates. VA researchers and experts who reviewed the data for The Times said there were myriad possibilities, including whether the military had disproportionately drawn women at higher suicide risk and whether sexual assault and other traumatic experiences while serving played a role.
The VA suicide study involved data on 173,969 adult suicides in 23 states over 11 years, which included the deaths of 40,571 male vets and 2,637 female vets. The article in Psychiatric Services also says that that people who join the military are more likely to have had troubled childhoods; and it could be the case that women who signed up were at higher risk of suicide in the first place.
• While the percentage of all suicides reported as Veterans has decreased, the number of suicides has increased.
• A majority of Veteran suicides are among those age 50 years and older.
• Male Veterans who die by suicide are older than non-Veteran males who die by suicide.
• The age distribution of Veteran and non-Veteran women who have died from suicide is similar.
• The demographic characteristics of Veterans who have died from suicide are similar among those with and without a history of VHA service use.
• Among those at risk, the first 4 weeks following service require intensive monitoring and case management. • There is preliminary evidence in 2012 indicating a decrease in the rate of non-fatal suicide events for VHA utilizing Veterans.
• Decreasing rates of non-fatal suicide events are associated with increasing age.
• The data show a decrease in the 12 month re-event prevalence in fiscal year (FY) 2012.
• The majority of Veterans who have a suicide event were last seen in an outpatient setting.
• A high prevalence of non-fatal suicide events result from overdose or other intentional poisoning.
• Continued increases in calls to the Veterans Crisis Line may be associated with efforts to enhance awareness of VHA services through public education campaigns.
• The majority of callers to the Veterans Crisis Line are male and between the ages of 50- 59.
• Differences in the age composition of callers to the Veterans Crisis Line are associated with gender.
• A large percentage of callers to the Veterans Crisis Line are identified as Veterans.
• Approximately 19 percent of callers to the Veterans Crisis Line call more than once each month.
• The percentage of callers to the Veterans Crisis Line who are currently thinking of suicide has decreased.
• The percentage of all calls resulting in a rescue has decreased, indicating that the calls are less emergent and callers are using the Crisis Line earlier.
• The percentage of callers receiving a referral for follow-up care is increasing.
• Approximately 93 percent of all Veterans Crisis Line referrals are made to callers with a history of VHA service use in the past 12 months.
• Service use continues to increase following a referral for care.
• Between FY 2009 – FY 2011, use of inpatient and outpatient services increased following a rescue.
• The 12 month re-event prevalence has decreased among those who have been rescued or received a referral for follow-up care.
New Brain Discovery? Lymph!
The discovery may require a reassessment of our assumptions about lymph drainage in the brain and its role in diseases involving brain inflammation or degeneration, such as Alzheimer’s disease and multiple sclerosis. The study was published in the peer-reviewed scientific journal Nature.
When I was in medical school, we were taught that the central nervous system (brain and spinal cord) did not have a typical lymphatic drainage system. Lymph is the immune fluid that circulates through the body, containing white blood cells to fight infection and destroy abnormal cells. This study aimed to look at the circulation of lymph in the mouse brain, but mice and humans do not have identical biology, so the findings may not be directly applicable.
The study involved complex laboratory techniques, using a fluorescent antibody to assess the alignment of cells within the brain, examination for markers associated with a lymphatic drainage system and looking at the functional capacity of identified vessels to carry lymphatic fluid to and from the brain.
Human samples taken from the brain at autopsy were used to investigate any structures found in mice.
The scientists found that the outer protective layers of the mouse brain showed cells that were clearly lined up, which suggested that these were vessels with a unique function. These cells showed the characteristic features of functional lymphatic vessels. These vessels appeared able to carry both fluid and immune cells from the fluid surrounding the brain and spinal cord (the cerebrospinal fluid), and were connected to the lymph nodes in the neck. The location of these vessels may have been the reason they have not been discovered before, thereby causing the belief that there is no lymphatic drainage system in the brain.
This may mean current thinking about how the brain works needs to be reassessed. The researchers go on to say it could be the malfunction of these vessels that could be the cause of a variety of brain disorders, such as multiple sclerosis and Alzheimer’s disease.
Summary: This mouse study has examined the circulation of lymph in the brain. It discovered previously unknown lymphatic vessels in the outer layers of the mouse brain. If accurate, the findings may call for a review of how the immune system in the brain functions, and shed new light on its role in brain diseases involving brain inflammation or degeneration. Though animal research can give a good insight into biological and disease processes, and how they may work in humans, the processes in humans and mice are not identical. Further studies are needed to confirm these findings and to assess whether this knowledge is transferable to humans. As such, it is too early to say whether the findings could one day have any implications for the treatment of degenerative brain conditions such as multiple sclerosis or Alzheimer’s.
The original article in Nature can be found here.
Brain Scan Scams: Amen!
What the reader should understand is that Dr. Amen, like many promoters of fraudulent "cures," appeals to people who are vulnerable to snake-oil promotions and great salesmanship. He has even hornswoggled fellow entrepreneurial genius Rick Warren, best known for The Purpose Driven Life, and pastor of the Saddleback Church in California. Warren designated Amen as official guru for health and nutrition at his mega-church.
Few top researchers and scientists say that SPECT is anything but a research tool of limited clinical use in identifying strokes, brain injuries and the like. It is helpful in group studies, to say broad things about groups of patients, but not specific things about individual patients. And, researchers say, SPECT has largely since been surpassed by technologies such as PET and functional MRIs, which give images of far greater clarity. It’s no longer viewed as cutting edge.
The APA first debunked many of Amen’s SPECT claims in a 2005 report. In 2008, Carlat, the Tufts professor and author, went to California to test Amen’s clinic. He then wrote, in Wired Magazine, that the black-clad Amen looked “more like a Miami maitre d’ than a psychiatrist,” that the SPECT scan was “spectacularly meaningless” and that Amen’s analysis of it reminded him of a “shrewd palm reader.”
In 2010, Thomas Insel, director of the NIMH, wrote on his blog that while the technology “might be playing in prime time on some TV infomercials, brain-imaging experts say we’re not quite there yet.” Earlier this year, Anissa Abi-Dargham, a highly regarded professor of clinical psychiatry and radiology at Columbia who has done extensive work with brain imaging, spoke at an APA symposium on the limits of SPECT. She listened to Amen’s hour-long lecture there. Reached by phone recently, she said: “Had I known what this was, I would have never agreed to be part of it. It was not a scientific debate. It was propaganda for his clinics.”
No major research institution takes his SPECT work seriously, none regards him as “the number one neuroscience guy,” and his revelations, which he presents to rapt audiences as dispatches from the front ranks of science, make the top tier of scientists roll their eyes or get very angry. “In my opinion, what he’s doing is the modern equivalent of phrenology,” says Jeffrey Lieberman, APA presidentelect, author of the textbook “Psychiatry” and chairman of Psychiatry at Columbia University College of Physicians and Surgeons. (Phrenology was the pseudoscience, popular in the early 19th century, that said the mind was determined by the shape of the skull, particularly its bumps.) “The claims he makes are not supported by reliable science, and one has to be skeptical about his motivation.” “I think you have a vulnerable patient population that doesn’t know any better,” says M. Elizabeth Oates, chair of the Commission on Nuclear Medicine, Board of Chancellors at the American College of Radiology, and chair of the department of radiology at the University of Kentucky.
“A sham,” says Martha J. Farah, director of the Center for Neuroscience & Society at the University of Pennsylvania, summing up her thoughts on one of Amen’s most recent scientific papers. “I guess we’re all amateurs except for him,” says Helen Mayberg, a psychiatry, neurology and radiology professor at Emory School of Medicine and one of the most respected researchers into depression and brain scanning. “He’s making claims that are outrageous and not supported by any research.” “I can’t imagine clinical decisions being guided by an imaging test,” says Steven E. Hyman, former director of the National Institute of Mental Health and current director of the Stanley Center for Psychiatric Research at the Broad Institute of MIT and Harvard.
The APA, in fact, has twice issued papers that dispute “claims being made that brain imaging technology ... was useful for making a clinical diagnosis and for helping in treatment selections.” The most recent paper was the work of 12 doctors who spent three years assessing the latest research. The summary: “There are currently no brain imaging biomarkers that are currently clinically useful for any diagnostic category in psychiatry.”
Four years ago, Robert Burton, the author and former associate chief of the department of neurosciences at the University of California at Mount Zion Hospital, wrote a harsh article on Salon.com about Amen’s work. The headline was “Brain Scam.” When recently told that Amen was still in business and grossed $20 million last year, Burton asked for the dollar figure to be repeated. “Oh, my God,” he said. “Just oh, my God. At some point this gets to be obscene — that’s just my bias — but oh, my God.”
To read the entire article from The Washington Post, click here.
In 2010, concerns about Dr. Amen and the "brain scam industry" reached a boiling point. In The American Journal of Psychiatry, my colleague Dr. Bryon Adinoff wrote the following:
"Dr. Amen claims that numerous psychiatric illnesses can be diagnosed and treatments prescribed based on resting single photon emission computerized tomography (SPECT) images. Dr. Leuchter correctly points out the absence of empirical data to support the claims of Dr. Amen. Several years ago, following conversations with Dr. Amen on how to address such concerns, the Brain Imaging Council of the Society of Nuclear Medicine offered Dr. Amen the opportunity to submit his analyses of a blinded set of SPECT scans (to have been prepared by the Brain Imaging Council) to determine how effective his technique is at correctly diagnosing subjects. Although this proposed study could have provided support for his approach, the offer was declined. Nevertheless, for more than two decades, Dr. Amen has persisted in using scientifically unfounded claims to diagnose and treat patients (over 45,000 by his own count).
"There are several dangers to patients that can accrue from this approach: 1) patients (including children) are administered a radioactive isotope without sound clinical rationale; 2) patients pursue treatments contingent upon an interpretation of a SPECT image that lacks empirical support; and 3) based on a presumed diagnosis provided by Dr. Amen's clinics, patients are guided toward treatment that may detract them from clinically sound treatments.
"Just as serious is the danger to our field. It is likely that, within the next decade, Dr. Amen's claims will be realized in that psychiatrists will enjoy the ability to diagnose and prescribe treatments based, in part, upon neuroimaging findings. Unfortunately, if previously led astray by unsupported claims, patients and their doctors may be less inclined to utilize scientifically proven approaches once these are shown in the peer-reviewed literature to be effective.
"It is therefore incumbent upon all of us to monitor and regulate our field. We encourage physicians to remain vigilant of unproven approaches practiced by our peers and to immediately report these trespasses to their state medical boards."
Child Development and Brain Health
Someone with dyslexia may attend schools that recognize the deficit and help the child learn to read well; or they may have the help of a skilled educational psychologist who can work the magic and overcome the learning differences. On the other hand, someone who grows up in less fortunate circumstances, like living in poverty or suffering a broken home, may do very well if they are biologically resilient and strong. Problems arise, however, when some suffers biological vulnerability as well as a life short on developmental opportunity. When we see the chronically mentally ill, we often see the overlap of these two conditions.
New research suggests that family income, and to a lesser degree parental education, are associated with brain structure differences in children and young adults. Focusing on brain regions critical for language, memory, and executive function in participants aged three to 20 years, scientists found that small differences in income were associated with relatively large differences in brain surface area in young people from the lowest-income families. This effect was smaller in higher-income families. Higher income was also associated with better performance in tests of cognitive ability. Increased levels of parental education were also related to increased brain surface area, although this effect was smaller when compared to the influence of income.
Although these study results do not suggest that low-income children have poor cognitive function, they indicate that interventions to reduce family poverty may help reduce socioeconomic disparities in child development and achievement. The full text of the findings can be found here.
Part 2: Texas Holdem Poker, Human vs. AI
The competition was set up by the Carnegie Mellon University School of Computer Science, who created a poker-playing program named ‘Claudico’ and were looking for a significant test. The program, with the ability to “learn” as it played and thus is considered an “artificial” intelligence, is the first-of-its-kind in that it was created to play No Limit Texas Hold’em; every other poker playing computer created played the more-statistical Limit version of the game. Once the Carnegie Mellon staff nailed down the players – and the management of the Rivers Casino in Pittsburgh offered an exciting venue to play – the subjects set out on the 14-day competition.
From the start, the representatives of the human race – World Series of Poker bracelet winner and online wunderkindDoug ‘WCGRider’ Polk, Dong Kim, Jason Les and Bjorn Li – moved out to a financial edge that they wouldn’t relinquish. Playing a total of 80,000 hands of $50/$100 Heads Up No Limit Hold’em over the two-week period, the four men built up a $587,231 edge only a week into the play. They would seemingly ride that advantage over the last half of the competition and, once the results were announced on Friday, both sides crowed about their achievement.
When the final tallies were completed, the “Brains” in the competition had vanquished their “Artificial Intelligence” foe by the sizeable figure of $732,713. Leading the way was Li, who accounted for an astounding $528,033 of the total winnings amassed by the humans. Polk didn’t do badly either, racking up $213,671 in winnings and Kim slipped by ‘Claudico’ in taking slightly more than $70,000 in earnings. Only Les would disappoint the human race, dropping $80,482 to be the only one to lose to ‘Claudico’ by the money counts. (The four men divvied up a $100,000 prize provided by the Rivers Casino for their two weeks of work.)
The human players were a bit surprised at the skill that ‘Claudico’ demonstrated. “We know theoretically that artificial intelligence is going to overtake us one day,” Li said during the post-match celebration. “At the end of the day, the most important thing is that the humans remain on top for now.” Les, who had seen a previous version of ‘Claudico’ when it defeated professional players just last year, was stunned by the developers’ skills.
“The advances made in Claudico in just eight months were huge,” Les said, indicating that, at that rate of improvement, an Artificial Intelligence system might need only another year before it clearly plays better than professionals.
Polk seemed to be the only player who critiqued the playing of ‘Claudico’ during the finale. “There are spots where it plays well and others where I just don’t understand it,” Polk noted, stating that some of its bets were highly unusual. Polk saw instances that, where a human might place a bet worth half or three-quarters of the pot, Claudico would sometimes bet a miserly 10% or an over-the-top all-in move. “Betting $19,000 to win a $700 pot just isn’t something that a person would do,” Polk observed.
So who won the event? While the overall numbers would suggest that the “Brains” crushed the “Artificial Intelligence,” a closer look at those figures is necessary. As individuals, the humans once again take a 3-1 winning edge, but the actual analysis of the figures that the players put up indicate that the score might have been closer to 1-0-3, with Li the only outright winner and the remainder of the human team within the statistical range of calling their matches a tie. It wasn’t a point that was missed by the professor who helped to develop ‘Claudico.’
“We knew Claudico was the strongest computer poker program in the world, but we had no idea before this competition how it would fare against four Top 10 poker players,” said Dr. Tuomas Sandholm, the Carnegie Mellon University professor of computer science who helped to create ‘Claudico.’ “It would have been no shame for Claudico to lose to a set of such talented pros, so even pulling off a statistical tie with them is a tremendous achievement.” In replying to Polk’s stab at the unorthodox play during the event, the Carnegie Mellon team admitted they were just as puzzled as to why ‘Claudico’ made the decisions he made.
After the completion of the interesting competition, there have been no indications that there will be another event on the horizon. The Carnegie Mellon team will no doubt head back to the laboratory to tweak on ‘Claudico’ (or potentially a more-potent creation?), while the human race will wait for the next challenge to their ‘superiority’ in this world.
This may turn out to be the latest installment in a grand tradition of computers beating us at our own games. In 1997, IBM's Deep Blue computer famously beat chess great Garry Kasparov. Four years ago, IBM's Watson took part in the TV quiz show Jeopardy! and crushed two contestants with a strong track record. AI has even mastered the popular smartphone game 2048.
Still, poker is a tough nut to crack. In a game like chess, everyone knows where all the pieces are on the board. By contrast, poker is a game of imperfect information: players don't know for sure what cards the others hold or what will come up next in the deck. That makes it a challenge for any player, human or computer, to choose the right play.
(This blog entry was compiled from various sources, and some attribution is lacking. I apologize and will correct this if I can.)
Painkiller Overdoses On the Rise
This news isn’t shocking to those of us who encounter addiction daily, but it’s in the headline today at USA Today. Other items of note from today’s paper:
With nearly 44,000 deaths a year, more Americans today die from drug overdoses than from car accidents or any other type of injury. Many of these deaths could be prevented if patients had better access to substance abuse therapy, experts say. Yet people battling addiction say that treatment often is unavailable or unaffordable.
Only 11% of the 22.7 million Americans who needed drug or alcohol treatment in 2013 actually got it, according to the Substance Abuse and Mental Health Services Administration. While some of those who went without care did so by choice, at least 316,000 tried and failed to get treatment.
"We know addiction treatment saves lives, reduces drug use, reduces criminal activity and improves employment," says Paul Samuels, president and director of the Legal Action Center, which advocates on behalf of people with HIV or addiction. "The data is there, the evidence is in, but our public policy has not caught up with the science."
Meanwhile, the crisis is getting worse, says Thomas Frieden, director of the Centers for Disease Control and Prevention. The death rate from drug overdoses more than doubled from 1999 to 2013, according to the CDC. The bulk of these deaths involve opiates, a class of pain killers that includes morphine and Oxycontin.
Injection drug use has fueled an outbreak of HIV in rural Indiana, a nationwide surge in hepatitis C infections, and an increase in the number of babies born addicted to drugs. States have responded to the surge in overdose deaths by expanding access to naloxone, a fast-acting rescue drug that can reverse the effects of an opiate overdose. Indiana lawmakers also voted to allow needle exchange programs in communities facing a public health crisis related to injection drug use. While those approaches are welcome, they don't treat the underlying addiction.
The wait for a spot in a detoxification program ranges from days to weeks, and it can be very expensive. As I say elsewhere here on my site, it's also true that not all treatment is really good treatment. Consumers are disadvantaged twice. Not only is treatment hard to find in the first place, but it's hard to know what constitutes a good treatment program. I have some comments about this on my FAQ page and on my Philosophy page.
Part 1: Texas Holdem Poker, Human vs AI Computer
HUMAN VS. MACHINE AS TOP POKER PROS TAKE ON AI
Fifteen years ago I, Dr. John Talmadge, became a serious poker player. I have a winning record at the poker table, and although I am (probably) not good enough to quit my day job, I have held my own with professionals in Las Vegas, and I finished in the top third of the field in the World Series of Poker Senior Event in 2009. Although I finished out of the money, I came in ahead of about 2000 other players in that event. In the years since, I have consulted with professional players on "the mental game," and I remain a serious student of Texas Holdem, the world's greatest card game.
Now comes Aviva Rutkin, writing in New Scientist that human poker professionals are taking on artificial intelligence (and the strongest poker playing computer built to date), and they are playing for real money. Here's the story.
Computer scientists have already made some progress, at least with simpler forms of the game. But the version being played at the Pittsburgh tournament, called Heads Up No Limit Texas Hold 'em, is "a completely different beast", says pro player Vanessa Selbst. "There's much more human elements and game strategies to employ, so it's a much more complex game." What's more, there are no betting limits, so the computer also has to take into account how much players might stake on each game.
Competing in Pittsburgh is Claudico, a program created at Carnegie Mellon University. Claudico taught itself poker skills by playing trillions of games in search of some kind of optimal strategy. Whatever it has picked is pretty good: last year, Claudico beat all 13 other computer competitors at no-limit poker in the annual contest run by the Association for the Advancement of Artificial Intelligence.
Computers have a few edges over humans, says graduate student Noam Brown, part of the team behind Claudico. For example, a computer can switch randomly between various betting strategies, which may confuse human opponents.
On the other hand, Claudico is slow to pick up on and adapt to people's playing styles – something that many pro players do with ease. "One of our big concerns is that the human will be able to identify weaknesses that Claudico has and exploit them," says Brown.
Because Claudico taught itself to play, even the team that built it don't quite know how it picks its moves. "We're putting our faith in Claudico. It knows much better than we do what it's doing."
Algorithms like those used to play poker could be valuable for other kinds of problems characterised by imperfect information. They could suggest optimal locations for military resources in a war, for example. Rival AIs could also be tasked to negotiate with each other over insurance rates or handle legal squabbles. "In society, sometimes you see one side getting screwed over because someone has more lawyers or more information or more resources at their disposal," says Brown. "Something like this can really level the playing field."
The winner of the poker tournament won't be crowned until the event ends on 7 May. Eric Jackson, a software engineer who creates poker bots as a hobby, is cautiously optimistic that Claudico can win. As we went to press, the pros and Claudico were neck and neck.
Even if AI triumphs, it won't mean programmers have conquered the game. "Beating humans decisively would be a landmark, but it wouldn't mean the end of work on poker," says Jackson. "We still don't know what the perfect strategy is."
The original article by Aviva Rutkin can be found online here.
Traumatic Brain Injury: Progress
"Gist reasoning characterizes a meaningful, complex cognitive capacity. Assessing how well one understands and expresses big ideas from information they are exposed, commonly known as an ability to "get the gist", is window into real life functionality. I do not know of any other paper and pencil test that can tell us both," explained Asha Vas, Ph.D., research scientist at the Center for BrainHealth and lead study author. "Although performance on traditional cognitive tests is informative, widely-used measures do not paint the full picture. Adults with TBI often fare average or above on these structured measures. All too often, adults with brain injury have been told that they ought to be fine; in reality, they are not doing and thinking like they used to prior to the injury and struggle managing everyday life responsibilities years after the injury. Gist reasoning could be a sensitive tool to connect some of those dots as to why they are having trouble with real-life functionality despite falling into the range of "normal" on other cognitive tests." For more details and the longer article, click here.
Kevin McCauley, M.D. on Addiction
Aging Brain? Not So Bad...
At middle age, the brain begins to draw on more of its capacity for improved judgment and decision making.
If you forget a name or two, take longer to finish the crossword, or find it hard to manage two tasks at once, you’re not on the road to dementia.
What you’re experiencing is your brain changing the way it works as you get older. And in many ways it’s actually working better. Studies have shown that older people have better judgment, are better at making rational decisions, and are better able to screen out negativity than their juniors are.
Although it may take you a little longer to get to the solution, you’re probably better at inductive and spatial reasoning at middle age than you were in your youth.
The brain changes as we get older, and in some ways it works better as we get older.
How is it possible for older people to function better even as their brains slow? “The brain begins to compensate by using more of itself,” explains Dr. Bruce Yankner, professor of genetics and co-director of the Paul F. Glenn Laboratories for the Biological Mechanisms of Aging at Harvard Medical School. He notes that MRIs taken of a teenager working through a problem show a lot of activity on one side of the prefrontal cortex, the region we use for conscious reasoning. In middle age, the other side of the brain begins to pitch in a little. In seniors, both sides of the brain share the task equally. The cooperative effort has a payoff. “Several studies suggest that seniors who can activate both sides of the brain actually do better on tasks, while those who can’t do worse,” Dr. Yankner says.
If you’ve found that it’s a little harder to carry on a conversation while searching your bag for your keys, MRI studies offer some clues. They show that in younger people, the area of the brain used to do a task goes dark immediately once the task is completed, while in older people it takes longer to shut down. As a result, it’s harder for the older brain to take on several tasks, because not only do you need to use more of the brain for any single task, but the brain also has a harder time letting go of a task. So even after you fish out your keys, you may have trouble getting back into the conversation.
What about the moments when you find yourself driving down the street without any recollection of having passed the last few blocks? Or the times you’ve locked the car door with your keys in the ignition? On those occasions your brain may have slipped into the default mode, which controls processes like remembering and daydreaming that are not required for a directed task. Imaging studies show that interconnected regions of the brain dubbed the “default network” grow more active with age, indicating that as we age we spend more time daydreaming.
THE GOOD NEWS ABOUT "THE MORE MATURE" BRAIN
At The Center for BrainHealth, as at Harvard, we are discovering that the more mature brain actually has advantages over its younger counterpart. These findings came as a surprise to many people, who were accustomed to seeing “senior moments”—groping for the right word or taking longer to articulate your thoughts—as a sign that the brain was on the skids. Yet even in professions where youth is valued, testing has shown that maturity has advantages.
For example, in a study of air-traffic controllers and airline pilots, those between ages 50 and 69 took longer than those under 50 to master new equipment, but once they had, they made fewer mistakes using it. (Keep this in mind when you’re trying to conquer a new computer program or adapt to a new car!) The mastery that comes with maturity is due to changes in your glands as well as your brain. Declining levels of testosterone—even in women—result in better impulse control. The end of the hormonal roller coaster of menopause may also contribute to emotional stability. After midlife, people are less likely to have emotional issues like mood swings and neuroses that interfere with cognitive function.
Most importantly, the wealth of knowledge from decades of learning and life experience enables you to better assess new situations. At midlife, most people are more adept at making financial decisions and getting to the heart of issues than they were when they were younger.
In most people, these abilities improve with age:
Inductive reasoning. Older people are less likely to rush to judgment and more likely to reach the right conclusion based on the information. This is an enormous help in everyday problem solving, from planning the most efficient way to do your errands to managing your staff at work.
Verbal abilities. In middle age, you continue to expand your vocabulary and hone your ability to express yourself.
Spatial reasoning. Remember those quizzes that require you to identify an object that has been turned around? You are likely to score better on them in your 50s and 60s than you did in your teens. And you may be better at some aspects of driving, too, because you are better able to assess the distance between your car and other objects on the road.
Basic math. You may be better at splitting the check and figuring the tip when you’re lunching with friends, simply because you’ve been doing it for so many years.
Accentuating the positive. The amygdala, the area of the brain that consolidates emotion and memory, is less responsive to negatively charged situations in older people than in younger ones, which may explain why studies have shown that people over 60 tend to brood less.
Attaining contentment. Years ago, researchers were surprised to find that people seem to be more satisfied with their lives as they age, despite the losses that accumulate with passing years. This is probably because they tend to minimize the negative, accept their limitations and use their experience to compensate for them, and set reasonable goals for the future. Dr. Yankner notes that this trait may be innate, because it is prevalent even in the United States and other Western nations, which tend to value youth over age.
Network Adequacy: Not Adequate
Deceptive insurance company practices
According to Mark Moran, writing in the April 3, 2015 issue of Psychiatric News, access to psychiatry appears to be an area in which many health plans are offering deceptive products. This problem has been studied for many years in Maryland, near the nation's capital, where access to care has long been a troubled business. Previous studies done over the last 25 years by MHAMD and other organizations found there were long delays for individuals to access psychiatric care. In 1988, MHAMD published, “Study of Mental Health Coverage Provided by Maryland HMOs.”
This study sought to provide a comprehensive picture of the impact of HMOs on access to mental health care. The anecdotes from mental health professionals in 1988 illustrated the long wait times their patients faced when trying to secure an appointment with a psychiatrist. As a follow-up, in 2002, the Mental Health Coalition of Maryland conducted a survey of mental health professionals to ascertain how the managed care system affected an individual’s ability to access mental health care.
Psychiatrists dropping our of private insurance networks
Many respondents reported dropping out of private insurance networks, resulting in more consumers having to pay out of pocket for mental health care. In 2007, the Maryland Psychological Association published a white paper titled, “Access to Care in the State of Maryland.” Their survey found that 44% of mental health professionals listed in the managed care networks were unreachable, and that the average wait time for an appointment with a psychiatrist was 25 days.
In the same April 2015 article, attorney Colleen Coyle, general counsel for the American Psychiatric Association, said that "in many instances health plans advertise provider networks that appear to offer users of behavioral health services a wide range of option for access to care, but in reality those networks may be much "thinner" than consumers are led to believe.
Insurance false advertising is fraud
"In my view, that is fraud," Coyle said. The insurer is promoting a provider list that it knows is not reflective of the access to care that patients will really have. I don't think it's innocent at all."
She goes on to say that insurance plans are constantly looking at their providers and and claims "because that's how they target which providers to audit and whether they are going to challenge the claim."
John McIntyre, M.D., a past president of the American Medical Association, said: "Many insurers, in an attempt to hold down costs, employ very narrow or shallow networks that are inadequate to provide necessary medical care. But patients don't know that when they sign up."
The detailed report from The Maryland Mental Health Association is available online here.
Best Therapists = Best Outcomes (by far)
Treatment: Know What to Ask
SEEKING TREATMENT: KNOW WHAT TO ASK
My goal in helping people includes educating them about what questions to ask.
Finding the right treatment for a person’s specific needs is critical. And finding the right treatment is not easy. Drug and alcohol addiction treatment is not “one size fits all.”
Treatment outcomes depend upon:
- the extent and nature of the person’s problems;
• the appropriateness of treatment; - the competence and skill of clinical staff;
• the availability of additional services; and
• the quality of interaction between the person and the treatment providers.
Family and friends play important roles in motivating people with drug problems to enter and remain in treatment. However, trying to identify the right treatment programs for a loved one can be a difficult process.
The National Institute on Drug Abuse (NIDA) has sound advice about the five questions to ask when searching for a treatment program:
1. Does the program use treatments backed by scientific evidence?
In the internet era, answering this question has become increasingly difficult. Many programs offer flashy "treatments" that are not scientific at all, despite claims made on beautiful web pages. According to Thomas McLellen, professor of psychiatry at the University of Pennsylvania, 90% of patients who enter addiction treatment programs don’t receive evidence-based treatment. Many current programs actually reject scientific evidence. For example, they prohibit the use of addiction medications, even though they’ve been shown to be more effective treating some addictions (specifically, the range of opiates like Oxycontin to heroin) than anything else. My concern is a bit different from Dr. McLellan's view (for example, he is not friendly toward 12 Step work). My major concern is that there are dozens of quack therapies, ranging from nutritional "cures" to "new age" approaches, to potentially harmful "trauma therapy."
A great website is not a guarantee that the advertised program is any good at all. Many programs today, using clever marketing, take advantage of opposition to Alcoholics Anonymous and 12 Step Programs by advertising that says, "We are NOT a 12 Step Program!" What these programs fail to do, in almost every example, is to state clearly what they actually do in their approach. Many other websites—and I have reviewed hundreds of them—claim to offer "evidence based treatment," when in fact the program is not evidence based at all. The average person has no idea whether or not claims of scientific evidence are true. Above all, beware of "testimonials" and celebrity endorsements. In selecting a treatment program, you have to use at least as much good judgment as you would use if you were buying a new car or having heart surgery.
Effective alcoholism and addiction treatments can include cognitive behavioral therapy, medications, or, ideally, the combination of both.
Key elements include:
• addressing a patient’s motivation to change;
• providing incentives to stop drinking or using drugs;
• building skills to resist alcohol/drug use;
• replacing addiction related activities with constructive and rewarding activities;
• improving problem-solving skills; and
• building better personal relationships.
Any and every good addiction treatment program will include competent assessment by a qualified addiction psychiatrist. Some programs will team an addiction medicine doctor with a well-qualified clinical psychologist, and that can work well. The point is that everything begins with getting the right assessment. Medications are an important part of treatment for many patients, especially when combined with counseling and other behavioral therapies. Different types of medications may be useful at different stages of treatment: to stop alcohol and drug abuse, to stay in treatment, and to avoid relapse.
2. Does the program tailor treatment to the needs of each patient?
No single treatment is right for everyone. The best treatment addresses a person’s various needs, not just his or her alcohol and drug abuse. Matching treatment settings, programs, and services to a person’s unique problems and level of need is key to his or her ultimate success in returning to a productive life. It is important for the treatment approach to be broad in scope, taking into account a person’s age, gender, ethnicity, and culture. The severity of addiction and previous efforts to stop using drugs can also influence a treatment approach.
The best programs provide a combination of therapies and other services to meet a patient’s needs. In addition to addiction treatment, a patient may require other medical services, family therapy, parenting support, job training, and social and legal services.
Finally, because addictive disorders and other mental disorders often occur together, a person with one of these conditions should be assessed for the other. And when these problems co-occur, treatment should address both (or all conditions), including use of medications, as appropriate.
Medical detoxification is a necessary first step in the treatment of certain addictions, but by itself does little to change long-term drug use.
3. Does the program adapt treatment as the patient’s needs change?
Individual treatment and service plans must be assessed and modified as needed to meet changing needs.
A person in treatment may require varying combinations of services during its course, including ongoing assessment. For instance, the program should build in drug monitoring so the treatment plan can be adjusted if relapse occurs. For most people, a continuing care approach provides the best results, with treatment level adapted to a person’s changing needs. A patient’s needs for support services, such as day care or transportation, should also be met during treatment.
4. Is the duration of treatment sufficient?
Remaining in treatment for the right period of time is critical. Appropriate time in treatment depends on the type and degree of a person’s problems and needs. People argue about this point all the time, and I don't have the patience or space on this blog to cite the references, but research tells us that most addicted people need at least three months in treatment to really reduce or stop their drug use and that longer treatment times result in better outcomes. The best programs will measure progress and suggest plans for maintaining recovery. Recovery from drug addiction is a long-term process that often requires several episodes of treatment and ongoing support from family or community. If you have read this far and are starving for the references, contact me.
Relapse does not mean treatment failure. The chronic nature of addiction means that relapsing to drug abuse is not only possible, but likely, similar to what happens with other chronic medical illnesses—such as diabetes, hypertension, and asthma—that have both physical and behavioral components. And like these illnesses, addiction also requires continual evaluation and treatment modification if necessary. A relapse to drug use indicates a need to re-instate or adjust treatment strategy; it does not mean treatment has failed.
5. How do 12-step or similar recovery programs fit into drug addiction treatment?
Self-help groups can complement and extend the effects of professional treatment. The most well-known programs are Alcoholics Anonymous (AA), Narcotics Anonymous (NA), and Cocaine Anonymous (CA), all of which are based on the 12-step model. This group therapy model draws on the social support offered by peer discussion to help promote and sustain drug-free lifestyles.
Most drug addiction treatment programs encourage patients to participate in supportive therapy during and after formal treatment. These groups offer an added layer of community-level social support to help people in recovery with abstinence and other healthy lifestyle goals.
To order NIDA materials, please go to: http://drugpubs.drugabuse.gov.
Being Mindful: Getting Started
Find a good spot in your home or apartment, ideally where there isn’t too much clutter and you can find some quiet. Leave the lights on or sit in natural light. You can even sit outside if you like, but choose a place with little distraction.
At the outset, it helps to set an amount of time you’re going to “practice” for. Otherwise, you may obsess about deciding when to stop. If you’re just beginning, it can help to choose a short time, such as five or ten minutes. Eventually you can build up to twice as long, then maybe up to 45 minutes or an hour. Use a kitchen timer or the timer on your phone. Many people do a session in the morning and in the evening, or one or the other. If you feel your life is busy and you have little time, doing some is better than doing none. When you get a little space and time, you can do a bit more.
Take good posture (see instructions above with actor Sandra Oh above) in a chair or on some kind of cushion on the floor. It could be a blanket and a pillow, although there are many good cushions available that will last you a lifetime of practice. You may sit in a chair with your feet on the floor, loosely cross-legged, in lotus posture, kneeling—all are fine. Just make sure you are stable and erect. If the constraints of your body prevent you from sitting erect, find a position you can stay in for a while.
When your posture is established, feel your breath—or some say “follow” it—as it goes out and as it goes in. (Some versions of the practice put more emphasis on the outbreath, and for the inbreath you simply leave a spacious pause.) Inevitably, your attention will leave the breath and wander to other places. When you get around to noticing this—in a few seconds, a minute, five minutes—return your attention to the breath. Don’t bother judging yourself or obsessing over the content of the thoughts. Come back. You go away, you come back. That’s the practice. It’s often been said that it’s very simple, but it’s not necessarily easy. The work is to just keep doing it. Results will accrue.
The Brain: A Good Introduction
The brain is the most complex organ in the human body. It produces our every thought, action, memory, feeling and experience of the world. This jelly-like mass of tissue, weighing in at around 1.4 kilograms, contains a staggering one hundred billion nerve cells, or neurons.
The complexity of the connectivity between these cells is mind-boggling. Each neuron can make contact with thousands or even tens of thousands of others, via tiny structures called synapses. Our brains form a million new connections for every second of our lives. The pattern and strength of the connections is constantly changing and no two brains are alike.
It is in these changing connections that memories are stored, habits learned and personalities shaped, by reinforcing certain patterns of brain activity, and losing others. To read the article, click here.
New Videos Added Today
4/26/2015
New in the media section: videos by Dr. Sandi Chapman, Dr. Ian Robertson, Dr. Howard Somers. Topics include a TED talk, an interview with the parents of a distinguished veteran who committed suicide, and a talk on "The Winner Effect."
Those Danged Cognitive Distortions
1. ALL-OR-NOTHING THINKING: You see things in black-and-white categories. If performance falls short of perfect, you see yourself or others as total failures.
2. OVERGENERALIZATION: You see a single negative event as a never-ending pattern of defeat. Phrases like "You always …" or "You never …" exemplify overgeneralization.
3. MENTAL FILTER: You pick out a single negative detail and obsess on it so that your vision of all reality becomes darkened, like the drop of ink that discolors an entire glass of water.
4. DISQUALIFYING THE POSITIVE: You reject positive experiences by insisting they "don't count" for some reason or other. In this way you can maintain a negative belief that is contradicted by your everyday experiences. Often this manifests as making excuses when somebody pays you a compliment.
5. JUMPING TO CONCLUSIONS: You make a negative interpretation even though there are no definite facts that convincingly support your conclusion often a "wait and see" attitude is called for in these situations.
• MIND READING: You arbitrarily conclude (usually by personalizing their behavior) that someone is reacting negatively to you, and you don't bother to check this out.
• THE FORTUNE TELLER ERROR: You often anticipate that things will turn out badly, and you feel convinced that your prediction is an already-established fact.
6. MAGNIFICATION (CATASTROPHIZING) OR MINIMIZATION: You exaggerate the importance of things (such as your achievements or someone else's goof up), or you inappropriately shrink things until they appear tiny (your own character defects or other people's acceptable behavior). This is also called the "binocular trick."
7. EMOTIONAL REASONING: You allow your negative emotions to color how you see the world with an "I feel it, therefore it must be true."
8. SHOULD STATEMENTS: You try to motivate yourself or others with should and shouldn't, as if needing be whipped and punished before you could be expected anything. "Musts" and "oughts" are also offenders. The emotional consequences are guilt. When you
direct should statements toward others, you feel anger, frustration, and resentment as do they!
9. LABELING AND MISLABELING: This is an extreme form of overgeneralization. Instead of describing your error, you attach a negative label to yourself. "I'm a loser." When someone else's behavior rubs you the wrong way, you attach a negative label to him "He's a dumb jerk!" Mislabeling involves describing an event with language that is highly colored and
emotionally loaded, and generally not factually descriptive.
10. PERSONALIZATION: You see yourself as the cause of some negative external event, which in fact you were not primarily responsible for.
My generation of psychiatrists was the first to break with the old-fashioned, unscientific model known as Freudian psychoanalysis—the stereotype of the patient lying on the couch for years and being "analyzed" by the shrink. For some reason, our generation just didn't see this as very helpful or useful. Psychoanalysis in its pure form means 4-5 visits a week to the psychoanalyst, and the typical course of therapy is measured in years! There were no outcome studies proving the effectiveness of this approach. We really wanted something that would produce results, and an approach that the average person could afford.
Dr. Ben Martin at PsychCentral describes the new, scientific talk therapy this way: Cognitive behavioral therapy (also known by its abbreviation, CBT) is a short-term, goal-oriented psychotherapy treatment that takes a hands-on, practical approach to problem-solving. Its goal is to change patterns of thinking or behavior that are behind people’s difficulties, and so change the way they feel. It is used to help treat a wide range of issues in a person’s life, from sleeping difficulties or relationship problems, to drug and alcohol abuse or anxiety and depression. CBT works by changing people’s attitudes and their behavior by focusing on the thoughts, images, beliefs and attitudes that we hold (our cognitive processes) and how this relates to the way we behave, as a way of dealing with emotional problems.
An important advantage of cognitive behavioral therapy is that it tends to be short, taking four to seven months for most emotional problems. Clients attend one session per week, each session lasting approximately 50 minutes. During this time, the client and therapist are working together to understand what the problems are and to develop a new strategy for tackling them. CBT introduces them to a set of principles that they can apply whenever they need to, and which will stand them in good stead throughout their lives.
Cognitive behavioral therapy can be thought of as a combination of psychotherapy and behavioral therapy. Psychotherapy emphasizes the importance of the personal meaning we place on things and how thinking patterns begin in childhood. Behavioral therapy pays close attention to the relationship between our problems, our behavior and our thoughts.
Yoga for PTSD in the Military
Notes on Club Drugs
How Are Club Drugs Abused?
GHB and Rohypnol are available in odorless, colorless, and tasteless forms that are frequently combined with alcohol and other beverages. Both drugs have been used to commit sexual assaults (also known as “date rape,” “drug rape,” “acquaintance rape,” or “drug assisted” assault) due to their ability to sedate and incapacitate unsuspecting victims, preventing them from resisting sexual assault.
GHB is usually ingested orally, either in liquid or powder form, while Rohypnol is typically taken orally in pill form. Recent reports, however, have shown that Rohypnol is being ground up and snorted. Both GHB and Rohypnol are also abused for their intoxicating effects, similar to other CNS depressants. GHB also has anabolic effects (it stimulates protein synthesis) and has been used by bodybuilders to aid in fat reduction and muscle building. Ketamine is usually snorted or injected intramuscularly.
How Do Club Drugs Affect the Brain?
GHB acts on at least two sites in the brain: the GABA receptor and a specific GHB binding site. At high doses, GHB’s sedative effects may result in sleep, coma, or death. Rohypnol, like other benzodiazepines, acts at the GABA receptor. It can produce anterograde amnesia, in which individuals may not remember events they experienced while under the influence of the drug.
Ketamine is a dissociative anesthetic, so called because it distorts perceptions of sight and sound and produces feelings of detachment from the environment and self. Ketamine acts on a type of glutamate receptor (NMDA receptor) to produce its effects, which are similar to those of the drug PCP. Low dose intoxication results in impaired attention, learning ability, and memory. At higher doses, ketamine can cause dreamlike states and hallucinations; and at higher doses still, ketamine can cause delirium and amnesia.
Addictive Potential
Repeated use of GHB may lead to withdrawal effects, including insomnia, anxiety, tremors, and sweating. Severe withdrawal reactions have been reported among patients presenting from an overdose of GHB or related compounds, especially if other drugs or alcohol are involved.
Like other benzodiazepines, chronic use of Rohypnol can produce tolerance, physical dependence, and addiction.There have been reports of people binging on ketamine, a behavior that is similar to that seen in some cocaine or amphetamine dependent individuals. Ketamine users can develop signs of tolerance and cravings for the drug.
What Other Adverse Effects Do Club Drugs Have on Health?
Uncertainties about the sources, chemicals, and possible contaminants used to manufacture many club drugs make it extremely difficult to determine toxicity and associated medical consequences. Nonetheless, we do know that: Coma and seizures can occur following use of GHB. Combined use with other drugs such as alcohol can result in nausea and breathing difficulties. GHB and two of its precursors, gamma butyrolactone (GBL) and 1,4 butanediol (BD), have been involved in poisonings, overdoses, date rapes, and deaths. Rohypnol may be lethal when mixed with alcohol and/or other CNS depressants. Ketamine, in high doses, can cause impaired motor function, high blood pressure, and potentially fatal respiratory problems.
What Treatment Options Exist?
Not many. These drugs are exotic and relatively rare compared to alcohol, meth, cocaine, marijuana, commonly abused prescription medications. As far as I know, there are no treatment programs specifically devoted to club or designer drugs. This can be a problem for the addict or drug abuse seeking help for these drugs. They enter residential or outpatient programs where other patients, and often most of the staff, don't know or understand the problems unique to this group of chemicals. My recommendation is for careful initial assessment—I discuss this at length in both the FAQ section and my philosophy of treatment section—so that an intelligent and individualized treatment approach is possible, and so the right intensive treatment program is selected when needed.
SMART Training for Teens
Teen SMART Camp is a great chance for your children or grandchildren to boost their frontal lobe functioning and gain important strategies for learning.
For questions and registration, please contact Lindsay Gehan at Lindsay.Gehan@utdallas.edu or 972.883.3310
Over the last six years, BrainHealth researchers have trained more than 27,000 students in SMART through research grants. Results have shown significant changes in frontal lobe regions responsible for higher order thinking and problem solving after only 10 hours of training. SMART has shown substantial improvements in academic performance in those who have participated to date.
SMART is a series of seven cognitive strategies that can be applied to any learning context. As students’ progress through these steps, they learn to discard unsuccessful and superficial learning styles and to adopt a more robust, focused, and deeper-level strategic learning approach. Upon completion of the SMART training, students can apply the methodology to any subject and have been shown scientifically to do so over an extended period of time with success.
This summer’s teens will begin SMART Camp by receiving comprehensive strategy instruction, teaching them to use their brains more efficiently to improve learning. SMART campers employ their new strategies in a variety of fun learning activities involving academic content as well as personally-relevant materials such as their favorite song lyrics, television shows, magazine articles, or movies, emphasizing organizational and motivational skills. The training is designed to help the teens apply their newly learned strategies to everyday situations. Each camper works on an individual and a group project over the course of the camp to practice planning, goal setting and time management.
The brain is primed for higher order reasoning beginning in adolescence. As a result, this SMART program is offered for students who will enter the 7th through 12th grade in Fall 2015.
SMART Camp has a maximum enrollment of 20 students and are filled on a first-come, first serve basis. The full payment amount is due before the camp begins.
Schedule:
June 22-26th 2015 – The day will start promptly at 9:00 am and conclude at 3:00 pm.
SMART Camp takes place over one week at the Center for BrainHealth.
Please contact Lindsay Gehan at Lindsay.Gehan@utdallas.edu or 972-883-3310 for more information
Science on Will and Willpower - Part II
An excellent video of one of Roy's lectures is on my media page.
We try to control ourselves in all sorts of ways: eating right, exercising, avoiding drugs and alcohol, studying more, working harder, spending less. Baumeister says that the practical significance of all this is enormous. He says: "Most of the problems that plague modern individuals in our society — addiction, overeating, crime, domestic violence, sexually transmitted diseases, prejudice, debt, unwanted pregnancy, educational failure, underperformance at school and work, lack of savings, failure to exercise — have some degree of self control failure as a central aspect."
Baumeister goes on to say that two main traits that seem to produce an immensely broad range of benefits: intelligence and self-control. However, psychology has not found much one can do to produce lasting increases in intelligence. On the other hand, self-control can be strengthened, and the study of self-control is a rare and powerful opportunity for psychology to make a palpable and highly beneficial difference in the lives of ordinary people.
For example, in his research he has found that people perform relatively poorly on tests of self-control when they have engaged in a previous, seemingly unrelated act of self-control: "For instance, in a study in my lab, we invited some students to eat fresh-baked chocolate-chip cookies, and asked others to resist the cookies and munch on radishes instead. Then we gave them impossible geometry puzzles to solve. The students who ate the cookies worked on the puzzles for 20 minutes, on average. But the students who had resisted the tempting cookies gave up after an average of eight minutes."
"Such studies suggest," he continues, "that some willpower was used up by the first task, leaving less for the second. The pattern is opposite to what one would expect based on priming or activating a response mode. So we began to think that some kind of limited resource is at work: It gets depleted as people perform various acts of self-control. Over time, we have begun to link this resource to the folk notion of willpower."
Making decisions seems to use up our willpower. After making decisions, people perform worse at self-control. Conversely, after exerting self-control, decision-making shifts toward simpler and easier processes. That can lead people to make poorer decisions, or to avoid making choices at all. Apparently, decision making depletes the same resource as self-control.
One of Baumeister's examples of willpower depletion: "A dieter may easily avoid a doughnut for breakfast, but after a long day of making difficult decisions at work, he has a much harder time resisting that piece of cake for dessert. Another example might be losing your temper. Normally, you refrain from responding negatively to unpleasant things your romantic partner says. But if one day you’re especially depleted — maybe you’re trying to meet a stressful work deadline — and the person says precisely the wrong thing, you erupt and say the words you would have stifled if your self-control strength was at full capacity. What do you call this process? My collaborators and I use the term “ego depletion” to refer to the state of depleted willpower. Initially, we called it “regulatory depletion” because the first findings focused purely on acts of self-regulation. When it emerged that the same resource was also used for decision-making, we wanted a broader term that would suggest some core aspect of the self was depleted. We borrowed the term “ego” from Freudian theory because Freud had spoken about the self as being partly composed of energy and of processes involving energy."
In his book, Baumeister explains that some people imagine that self-control or willpower is something you only use once in a while, such as when you are tempted to do something wrong. The opposite is true. Research indicates that the average person spends three to four hours a day resisting desires. Self-control is used for other things as well: controlling thoughts and emotions, regulating task performance and making decisions. Most people use their willpower many times a day, all day. And toward the end of the day, there is less gas in the tank.
We now know that people can improve their self-control even as adults. As with a muscle, it gets stronger from regular exercise. So engaging in some extra self-control activities for a couple weeks produces improvement in self-control, even on tasks that have no relation to the exercise activities. The exercises can be arbitrary, such as using your left hand instead of your right hand to open doors and brush your teeth. Or they can be meaningful, such as working to manage money better and save more. The important thing is to practice overriding habitual ways of doing things and exerting deliberate control over your actions. Over time, that practice improves self-control. As people deplete willpower, they became increasingly likely to give in to desires they might otherwise have resisted. This was true for all manner of desires: desires to sleep, to eat, to have sex, to play games, to spend money, to drink alcohol or smoke cigarettes.
One of the best features of Roy Baumeister's work, particularly his book on willpower, is that he is easy to read, accessible to those of us not trained in clinical research or adept at deciphering scientific papers.
Addictionary: Language of Addiction
For example, when the word "alcohol" was written or spoken in early 19th-century America. it was often used in the chemical and medical sense. This is from an article about drawing out the essence of stramonium, or jimson weed: "The virtues of stramonium," the New England Journal of Medicine reported in January of 1818, "appear to be seated in an extractive principle, which dissolves in water and alcohol."
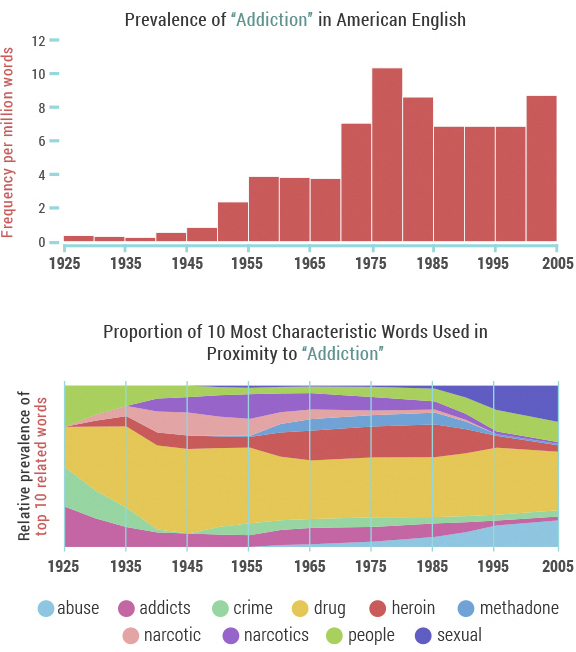
The word "cocaine" had different connotations as well. In the 1860s, for instance, a substance termed "cocaine" was advertised by a Boston company as a topical treatment to prevent hair loss.
Over time these words – "alcohol", "cocaine" and others, including "drugs" and" intoxicated" – became more closely associated with substance use, abuse and addiction in American popular culture.
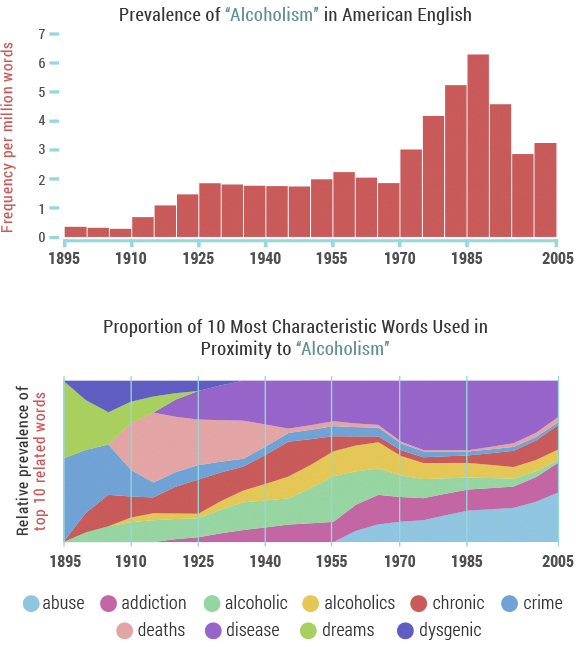
"'Alcoholism' made its debut in the lexicon around 1900, associated almost exclusively with 'crime' and 'dreams' – coincidentally around the time that Sigmund Freud's The Interpretation of Dreams was published," Recovery.org notes. "However, the association with crime was soon eclipsed by concern over 'chronic' alcoholism and 'death'/'deaths' related to alcoholism, which ballooned in the 1920s during the height of the prohibition movement." Documentarian Ken Burns echoes this in his series, Prohibition. One of the tragic unintended consequences of the nationwide crackdown on alcohol was an increase in dangerous, unregulated spirits — leading to 1,000 deaths a year.
Facebook, Twitter, and Linkedin
Videos Added to My Site
Genetics, Weird Facts, & Placebos
A placebo is anything that seems to be a "real" medical treatment -- but isn't. It could be a pill, a shot, or some other type of "fake" treatment. What all placebos have in common is that they do not contain an active substance meant to affect health. Younger physicians won't remember this, but years ago it was considered okay for doctors to prescribe placebos. Surgeons fairly often would substitute saline (salt water) injections when they worried that patients were asking for too many narcotic shots after an operation. There was a preparation called Gevrabon that was essentially sherry wine with some vitamins added, and it could be given by prescription "for relaxation at bedtime." Over the years, for obvious reasons, experts in medical ethics began to question whether these practices—essentially deceiving patients, but with good intentions—were proper and permissible.
In addiction medicine, I've seen college students come into the emergency room looking drunk, only to discover (with lab verification) that the "drug" they had tried was simply a vitamin pill. Similar findings have emerged at The University of Texas Austin, where one of the research labs has a full-fledged bar (i.e. a saloon) set up to simulate the settings where college students drink. Click here to see the Sahara Bar in the Department of Psychology. Study subjects sometimes get tipsy even when their margarita or manhattan contains no alcohol at all.
In 1996, scientists assembled a group of students and told them that they were going to take part in a study of a new painkiller, called "trivaricaine". Trivaricaine was a brown lotion to be painted on the skin, and smelled like a medicine. But the students were not told that, in fact, trivaricaine contained only water, iodine, and thyme oil – none of which are painkilling medicines. It was a fake – or placebo – painkiller. Read an abstract of the study: Mechanisms of Placebo Pain Reduction. With each student, the trivaricaine was painted on one index finger, and the other left untreated. In turn, each index finger was squeezed in a vice. The students reported significantly less pain in the treated finger, even though trivaricaine was a fake.
In this example, expectation and belief produced real results. The students expected the "medicine" to kill pain: and, sure enough, they experienced less pain. This is the placebo effect.
Placebo medicine has even been shown to cause stomach ulcers to heal faster than they otherwise would. These amazing results show that the placebo effect is real, and powerful. They mean that fake or placebo treatments can cause real improvements in health conditions: improvements we can see with our own eyes. Experiencing the placebo effect is not the same as being "tricked", or being foolish. The effect can happen to everyone, however intelligent, and whether they know about the placebo effect or not.
An article in Harvard Magazine describes Harvard Professor Dr.Ted Kaptchuk’s first randomized clinical drug trial, where nearly a third of his 270 subjects complained of awful side effects. All the patients had joined the study hoping to alleviate severe arm pain: carpal tunnel, tendinitis, chronic pain in the elbow, shoulder, wrist. In one part of the study, half the subjects received pain-reducing pills; the others were offered acupuncture treatments. And in both cases, people began to call in, saying they couldn’t get out of bed. The pills were making them sluggish, the needles caused swelling and redness; some patients’ pain ballooned to nightmarish levels. “The side effects were simply amazing,” Kaptchuk explains; curiously, they were exactly what patients had been warned their treatment might produce. But even more astounding, most of the other patients reported real relief, and those who received acupuncture felt even better than those on the anti-pain pill. These were exceptional findings: no one had ever proven that acupuncture worked better than painkillers. But Kaptchuk’s study didn’t prove it, either. The pills his team had given patients were actually made of cornstarch; the “acupuncture” needles were retractable shams that never pierced the skin. The study wasn’t aimed at comparing two treatments. It was designed to compare two fakes.
Dr. Kaptchuk and his colleagues have found that placebo treatments—interventions with no active drug ingredients—can stimulate real physiological responses, from changes in heart rate and blood pressure to chemical activity in the brain, in cases involving pain, depression, anxiety, fatigue, and even some symptoms of Parkinson’s. His work was also featured in a New Yorker article, "The Power of Nothing," that can be found here.
Here are four fascinating (and weird) facts about placebos and the placebo effect:
1. It doesn't have to be a secret. Some believe that a placebo can only work if the recipient is unaware they are taking one. But there's evidence that people with irritable bowel syndrome who knowingly receive a placebo do better than those who are left untreated.
2. It works better if it's expensive. The pain-killing power of a placebo pill is greater among people who are told they are taking a full-price version, compared to those told that the pill is on sale for a discounted price.
3. It's not just us, animals can get it too. A 2012 study found that between 30 and 40 per cent of rats experienced pain relief when their morphine injections were swapped for inactive saline solution.
4. It has an evil twin. The nocebo effect makes people undergoing treatment more likely to suffer from side-effects if they are warned about them by their doctor.
For the full New Scientist journal article on the subject, click here.
Slowly, over the past decade, researchers have begun to tease out the strands of the placebo response. The findings, while difficult to translate into medicine, have been compelling. In most cases, the larger the pill, the stronger the placebo effect. Two pills are better than one, and brand-name pills trump generics. Capsules are generally more effective than tablets, and injections produce a more pronounced effect than either. There is even evidence to suggest that the color of medicine influences the way one responds to it: colored pills are more likely to relieve pain than white pills; blue pills help people sleep better than red pills; and green capsules are the best bet when it comes to anxiety medication.
Mindfulness Based Relapse Prevention
Traditional treatment for substance abuse often focuses on avoiding or controlling triggers that result in negative emotion or craving. While research has shown that this approach can help, substance abuse relapse remains a problem: about half of those who seek treatment are using again within a year.
Bowen has spent much of her career studying another approach: mindfulness, which involves cultivating moment-to-moment, nonjudgmental awareness of thoughts, feelings, and surroundings. She and her colleagues have developed a program called Mindfulness-Based Relapse Prevention (MBRP), which combines practices like sitting meditation with standard relapse prevention skills, such as identifying events that trigger relapse. Rather than fighting or avoiding the difficult states of mind that arise when withdrawing from a substance, this combination tries to help participants to name and tolerate craving and negative emotion.
But how do mindfulness-based approaches compare to traditional substance abuse treatments? And do mindfulness-based treatments work for everyone? Researchers like Bowen are beginning to answer these questions.
Here is the key to the success of the program: MBRP helps people to relate differently to their thoughts, and use tools to disengage from automatic, addictive behaviors.
The JAMA Psychiatry article describes how effective the Mindfulness-Based Relapse Prevention program is in comparison to a standard relapse-prevention program as well as a conventional 12-step program. Six months following the intervention, the mindfulness-based program and the standard relapse-prevention program were both more successful at reducing relapse than the 12-step program. One year later, the mindfulness-based program proved better than the other two in reducing drinking and drug use.
Bowen says that when people cultivate mindfulness, they’re developing a tool to become aware of that inclination to want only pleasurable things and escape uncomfortable things. Mindfulness also helps people learn to relate to discomfort differently. When an uncomfortable feeling like a craving or anxiety arises, people like Sophia are able to recognize their discomfort, and observe it with presence and compassion, instead of automatically reaching for a drug to make it go away. Bowen says that awareness of our experience and the ability to relate to our experience with compassion gives us more freedom to choose how we respond to discomfort, rather than defaulting to automatic behaviors.
More research is needed to determine why MBRP might be more successful than other programs in reducing substance abuse relapse, but Bowen speculates that MBRP holds an advantage because mindfulness is a tool that can be applied to all aspects of one’s life.
Standard relapse-prevention programs teach tools specific to struggles with substance abuse—for instance, how to deal with cravings or how to say no when someone offers you drugs. A year after completing the program, a person may have a very different set of challenges that the relapse-prevention program did not equip them to deal with.
But because mindfulness is a tool that can be used in every part of a person’s life, practicing moment-to-moment awareness could continue to be an effective coping tool.
James Davis and his colleagues at Duke University are investigating mindfulness training as a way to help people quit smoking. Davis speculates that mindfulness is likely an effective tool in helping people with addiction because it’s a single, simple skill that a person can practice multiple times throughout their day, every day, regardless of the life challenges that arise. With so much opportunity for practice—rather than, say, only practicing when someone offers them a cigarette—people can learn that skill deeply.
Their intervention results showed a significant difference in smoking cessation for people who completed the intervention, as compared to people who were given nicotine patches and counseling from the Tobacco Quit Line.
Both Bowen and Davis emphasize that mindfulness is not a panacea; it doesn’t always work for everyone.
Dr. Zev Schuman-Olivier and his colleagues at the Massachusetts General Hospital Center for Addiction Medicine suggest that the type of therapy a person responds to may have something to do with their disposition. People who had the tendency to treat thoughts and behaviors with non-judgment and acceptance before the intervention began were more likely to be successful in reducing smoking following the mindfulness training. They write that if a person already has the skill to treat the self with non-judgment and acceptance, learning mindfulness practices likely comes easier to them than someone who has not previously practiced this skill.
Ultimately, the type of therapy that works best for a given person will likely capitalize on their pre-disposed strengths.Of course, as Bowen and Davis both note, the skills of mindfulness can be taught to everyone. But Schuman-Olivier’s finding suggests that people who are not oriented toward mindfulness may need a more vigorous or lengthy intervention, in order to more thoroughly learn mindfulness skills. It may be the case that people with less disposition toward mindfulness would fare better with a different therapy.
Another predictor of success in mindfulness-based treatment could be a person’s motivation to engage in the therapy. In Davis’ study, the people that started the intervention with the highest level of nicotine addiction were the most successful in reducing smoking by the end of the treatment. Davis said that this seemingly counterintuitive result likely reflects their motivation to quit; the people that were the most addicted had, at that point, tried everything, and were willing to try their hardest to make this therapy work. Meanwhile, people that were less addicted saw their addiction as less of a problem. They reasoned, “If this doesn’t work, I’ll be ok—something else will work, eventually.” As a result, they were likely less motivated to quit, and less engaged in the therapy.
Being Mindful and Positive
Mindfulness is natural, but we often overlook the importance of living in the present moment. There is not much new to learn; it's more about being aware of what is happening, who we are, and how to practice. We already have the capacity to be present, and it doesn’t require us to change who we are. You will hear me describe, in our conversations, topics like attention, awareness, empathy, compassion, being in the zone, situational awareness, presence, flow, contemplation, and many more. Being mindful has the power to change how we approach ourselves, our work, our relationships, and our communities. Mindfulness practice should be part of everyone's toolbox in the process of recovery from any mental or emotional setback. On my links page I have listed some useful resources on the subject.
Positive psychology began to emerge in the late 1980's through the research of my colleague Dr. Martin Seligman. If you have attended my talks on the positive psychology of addiction recovery, you've heard me describe "PERMA," the five dimensions of life where positive psychology produces meaningful results. Seligman outlines the categories in his book, Authentic Happiness. The acronym for the five elements of Seligman’s well-being theory is PERMA (Positive Emotions, Engagement, Relationships, Meaning and purpose, and Accomplishments).
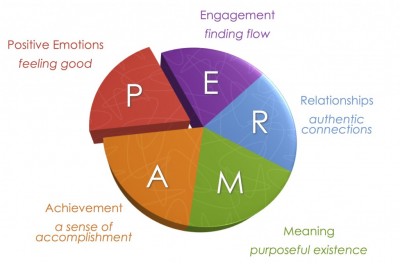
What people in addiction recovery notice, usually right away, is the strong similarity between the findings of positive psychology research and the guiding principles of twelve step recovery.
Positive emotions include a wide range of feelings, not just happiness and joy. Included are emotions like excitement, satisfaction, pride and awe, amongst others. These emotions are frequently seen as connected to positive outcomes, such as longer life and healthier social relationships.
Engagement refers to involvement in activities that draws and builds upon one’s interests. Mihaly Csikszentmihalyi explains true engagement as flow, a feeling of intensity that leads to a sense of ecstasy and clarity. The task being done needs to call upon higher skill and be a bit difficult and challenging yet still possible. Engagement involves passion for and concentration on the task at hand and is assessed subjectively as to whether the person engaged was completely absorbed, losing self-consciousness.
Relationships are all important in fueling positive emotions, whether they are work-related, familial, romantic, or platonic. We receive, share, and spread positivity to others through relationships. They are important in not only in bad times, but good times as well. In fact, relationships can be strengthened by reacting to one another positively. It is typical that most positive things take place in the presence of other people.
Meaning is also known as purpose, and prompts the question of “Why?” Discovering and figuring out a clear “why” puts everything into context from work to relationships to other parts of life. Finding meaning is learning that there is something greater than you. Despite potential challenges, working with meaning drives people to continue striving for a desirable goal. The three criteria are that it 1) contributes to well-being, 2) is pursued for its own sake, and 3) is measured independently of the other elements of PERMA.
Accomplishments are the pursuit of success and mastery. Unlike the other parts of PERMA, they are sometimes pursued even when it does not result in positive emotions, meaning, or relationships. Accomplishment can activate the other elements of PERMA, such as pride under positive emotion.Accomplishments can be individual or community based, fun or work based.
The five domains are valuable to consider when "the program isn't working," because taking personal inventory usually comes down to looking at what's going on inside these categories. The five elements were sifted out of research on thousands of individuals who were interviewed on the broad topic of happiness.
Change Your Brain
BRAINHEALTH PHYSICALS
A unique cognitive assessment that measures cognitive reserve in pivotal areas of higher-order mental functioning, all of which rely on robust frontal lobe function. It is just as essential to measure and monitor brain fitness as it is to measure and monitor physical fitness. Get a benchmark of your brain’s health.
HIGH PERFORMANCE BRAIN TRAINING
The high performance brain training program, Strategic Memory Advanced Reasoning Training (SMART®
I joined the staff at The Center for BrainHealth and BPI after extensive contact with the scientists and clinicians there. Over a period of months I found myself returning at least once or twice weekly to attend a lecture, to discuss research, or to interact with my friends on The Warrior Team, a powerful resource for veterans. I remember the day in November 2014 when I spoke with Dr. Sandra Chapman, the CEO, and she asked me whether I was enjoying my visits. "Are you kidding me?" I said, "I want to be more than a visitor—I want to work here!" Needless to say, I was both honored and extremely delighted when, early in 2015, I got the call and the invitation to be Senior Medical Advisor for CBH and BPI.
Brain Scams: Don't Buy the MRI
Dr. Carlat writes: "My journey through the land of functional neuroimaging has helped me to understand how spectacularly meaningless these images are likely to be. Most neuromarketers are using these scans as a way of sprinkling glitter over their products, so that customers will be persuaded that the pictures are giving them a deeper understanding of their mind. In fact, imaging technologies are still in their infancy. And while overenthusiastic practitioners may try to leapfrog over the science, real progress, which will take decades, will be made by patient and methodical researchers, not by entrepreneurs looking to make a buck."
If a person has a brain tumor, a brain aneurysm, or a stroke, then brain imaging can be helpful. However, brain imaging makes no difference (and makes no sense) in the treatment of problems like depression, anxiety, ADD/ADHD, alcoholism, addictions, or other commonly seen psychiatric disorders.
Brain imaging is very expensive, and the brain is exposed to radiation during a scan. This is an unnecessary risk, and a very expensive procedure, for anyone with a psychiatric disorder.
Beliefs Shape Our Reality
Surprisingly large numbers of people also hold beliefs that a psychiatrist would class as delusional. In 2011, psychologist Peter Halligan at Cardiff University assessed how common such beliefs were in the UK (see below for the top 10 delusions). He found that more than 90 per cent of people held at least one, to some extent. They included the belief that a celebrity is secretly in love with you, that you are not in control of some of your actions, and that people say or do things that contain special messages for you (Psychopathology, vol 44, p 106).
None of Halligan's subjects were troubled by their strange beliefs. Nonetheless, the fact that they are so common suggests that the "feeling of rightness" that accompanies belief is not always a reliable guide to reality.
The Top 10 Delusions
1. Your body, or part of your body, is misshapen or ugly 46.4%
2. You are not in control of some of your actions 44.3%
3. You are an exceptionally gifted person that others do not recognise 40.5%
4. Certain places are duplicated, i.e. are in two different locations at the same time 38.7%
5. People say or do things that contain special messages for you 38.5%
6. Certain people are out to harm or discredit you 33.8%
7. Your thoughts are not fully under your control 33.6%
8. There is another person who looks and acts like you 32.7%
9. Some people are duplicated, i.e. are in two places at the same time 26.2%
10. People you know disguise themselves as others to manipulate or influence you 24.9%
One of the most interesting things about belief is that it varies enormously from person to person, especially on issues that really matter such as politics and religion. According to research by Gerard Saucier of the University of Oregon, these myriad differences can be boiled down to five basic "dimensions" (Journal of Personality and Social Psychology, vol 104, p 921). At their core, he says, these concern what we consider to be worthy sources of value and goodness in life, whether it be a concept, an object, a supernatural being or a historical person. Your belief system is the aggregate of your position on each of these five dimensions, which are independent of each other.
1. Traditional religiousness: level of belief in mainstream theological systems such as Christianity and Islam
2. Subjective spirituality: level of belief in non-material phenomena such as spirits, astrology and the paranormal
3. Unmitigated self-interest: belief in the idea that hedonism is a source of value and goodness in life
4. Communal rationalism: belief in the importance of common institutions and the exercise of reason
5. Inequality aversion: level of tolerance of inequality in society, a proxy of the traditional left-right political split
To read the full article, click here.
Changing the Brain
People with chronic fatigue syndrome (CFS) tend to have a decrease in a type of brain tissue called grey matter in the prefrontal cortex of the brain. OCD researchers in the Netherlands provided 16 sessions of CBT, and found significant increases in gray matter volume in the prefrontal cortex. This seems to suggest that the CFS patients were able to “recover” some gray matter volume after CBT.
The bottom line: Although medication and psychotherapy appear to work their magic in difference places, the results are positive for both. The mechanism of action remains unclear, but studies also show that the combination of psychotherapy and the right medication (getting it right is very important!) is an excellent approach for many individuals. As the brain changes, we see the production of new proteins, which change our brains through neuroplasticity. In selecting a treatment strategy, sometimes medication works best, sometimes psychotherapy is the best option, and sometimes it’s a combination of the two.
What Is a Disease?
The ancient Greek academies had differing views of disease. Hippocrates emphasized the sick individual with his particular kind of misery. Others saw disease as a specific pathological process, evidenced by a visible sign such as a tumor, wound, or physical symptom. To this day, the definition of disease remains controversial. The AMA Council on Science and Public Health recently addressed the question, “Is obesity a disease?” The Council’s response: “Without a single, clear, authoritative, and widely accepted definition of disease, it is difficult to determine conclusively whether or not obesity is a medical disease state.”
This is also true for the vast majority of psychiatric disorders, particularly the addictions. The individual’s degree of suffering and incapacity—or distress and dysfunction—defines a state of disease. Although we now have some clues about the causes of mental disorders, and neuroimaging studies are making great strides, the American Psychiatric Association takes this position:
“The exact causes of mental disorders are unknown, but an explosive growth of research has brought us closer to the answers. We can say that certain inherited dispositions interact with triggering environmental factors. Poverty and stress are well-known to be bad for your health—this is true for mental health and physical health. In fact, the distinction between “mental” illness and “physical” illness can be misleading. Like physical illnesses, mental disorders can have a biological nature. Many physical illnesses can also have a strong emotional component.”
The National Alliance on Mental Illness (NAMI) seems to agree: “A mental illness is a condition that impacts a person's thinking, feeling or mood may affect and his or her ability to relate to others and function on a daily basis. Each person will have different experiences, even people with the same diagnosis. Recovery, including meaningful roles in social life, school and work, is possible, especially when you start treatment early and play a strong role in your own recovery process. A mental health condition isn’t the result of one event. Research suggests multiple, interlinking causes. Genetics, environment and lifestyle combine to influence whether someone develops a mental health condition. A stressful job or home life makes some people more susceptible, as do traumatic life events like being the victim of a crime. Biochemical processes and circuits as well as basic brain structure may play a role too.”
These questions highlight the importance of seeing the suffering person as more than a diagnosis or a label. This is the message I emphasize in my presentation, “Four Sides to Every Story,” available on request. Diagnosis is helpful, because we know that certain treatments are effective for certain diseases. For example, some fevers are caused by infection, and if we kill the offending bug we can cure the disease. Other fevers are caused by inflammation—as in rheumatoid arthritis or drug reactions—and if we calm the inflammation we can ease the fever.
At the same time, the psychiatrist should see much more than a label or a diagnosis (what the patient has in terms of the disease model). The psychiatrist—or any mental health professional—should also take the other three perspectives into account: who the person is, what the person does, and what the person has encountered. Using all four perspectives, the disease model can be valuable. It’s just not the whole story.
Painkillers, Narcotic Abuse, and Addiction
Over the past twenty years, drugs like hydrocodone, oxycontin, and similar narcotics have become an epidemic problem.
Opioids -- also called opiates or narcotics -- are pain relievers made from opium, which comes from the poppy plant. Morphine and codeine are the two natural products of opium. Synthetic modifications or imitations of morphine produce the other opioids:
Heroin (street drug)
Dilaudid (hydromorphone)
Percocet, Percodan, OxyContin (oxycodone)
Vicodin, Lorcet, Lortab (hydrocodone)
Demerol (pethidine)
Methadone
Duragesic (fentanyl)
When people use narcotics only to control pain, they are unlikely to become addicted to the drugs. However, opioids provide an intoxicating high when injected or taken orally in high doses. Opioids are also powerful anxiety relievers. For these reasons, narcotic abuse is one of the most common forms of drug abuse in the U.S.
Terms like opioid abuse, drug abuse, drug dependence, and drug addiction are often used interchangeably, but experts define them as follows:
Drug abuse, including opioid abuse, is the deliberate use of a medicine beyond a doctor's prescription. In the case of opiates, the intention is generally to get high or to relieve anxiety.
Dependence occurs when the body develops tolerance to the drug, meaning higher doses are needed for the same effect. In addition, stopping the drug produces drug withdrawal symptoms.
Drug addiction occurs when the person has drug dependence, but also displays psychological effects. These include compulsive behavior to get the drug; craving for the drug; and continued use despite negative consequences, like legal problems or losing a job.
Symptoms of Narcotic Abuse
Signs and symptoms of opioid abuse include:
- Analgesia (feeling no pain)
- Sedation
- Euphoria (feeling high)
- Respiratory depression (shallow or slow breathing)
- Small pupils
- Nausea, vomiting
- Itching or flushed skin
- Constipation
- Slurred speech
- Confusion or poor judgment
Symptoms of Opioid Drug Withdrawal
If a person uses opioids for a long time, they develop physical dependence and tolerance. Usually, opioid abusers will then take more of the drug, to continue to get high. If a person stops using opioids after they become physically dependent on the drug, they will experience drug withdrawal symptoms which can include:
Anxiety
Irritability
Craving for the drug
Rapid breathing
Yawning
Runny nose
Salivation
Gooseflesh
Nasal stuffiness
Muscle aches
Vomiting
Abdominal cramping
Diarrhea
Sweating
Confusion
Enlarged pupils
Tremors
Loss of appetite
I tell patients that withdrawal from drugs like painkillers and heroin is like the worst case of the flu you've ever experienced. The symptoms of opioid drug withdrawal can be agonizing and intolerable, contributing to continued drug abuse. In general, how severe opioid drug withdrawal symptoms are, and how long they last, depends on how long the person has been abusing opioids and how much they have been taking.
Medicines like methadone, buprenorphine (sometimes combined with naloxone), and naltrexone can be taken in various forms and are used to prevent withdrawal symptoms after a person stops using, a process called detoxification ("detox"). After drug withdrawal is complete, the person is no longer physically dependent on the drug. But psychological dependence can continue. Some people with drug addiction may relapse in response to stress or other powerful triggers.
Dependence vs. Addiction
Controlling pain is the goal when opioids are used medically. Patients or health care professionals should not let fear of addiction prevent them from using opioids for effective pain relief. Knowing the difference between dependence and addiction is important.
People who take opioids for pain relief for extended periods of time may need higher doses to ease their pain. They may develop tolerance to the drug and experience withdrawal symptoms if the medication is abruptly stopped. They become physically dependent on the drug.
Addiction occurs when narcotic abuse becomes compulsive and self-destructive, especially concerning an opioid user's need to use the drug for reasons other than pain relief.
To prevent withdrawal symptoms in people who have become physically dependent on opioids for pain relief, the dose may be slowly lowered over a few weeks. People who are weaned off opioids and are pain free usually don't start taking the drug again or become abusers of narcotics. Opioids used for short-term medical conditions rarely require weaning. In those cases, stopping the medication after a brief period usually doesn't cause withdrawal symptoms.
Other Abused Drugs
Strictly speaking, most drugs referred to informally as narcotics really aren't. However, two drug classes have some similar effects to opioids, when abused:
Benzodiazepines include Valium, Ativan, and Xanax. Benzodiazepine abuse results in sedation and calm, but tolerance develops rapidly. Withdrawal can result in seizures, unlike opioid withdrawal.
Barbiturates include Seconal, Amytal, Nembutal, and Luminal. Barbiturates are also sedating and calming. Withdrawal after continued barbiturate abuse, like benzodiazepine abuse, is medically serious.
In general, benzodiazepines and barbiturates have less pain-relieving effects than opioids. All three drug classes are sedating and anxiety-relieving. Benzodiazepine abuse, barbiturate abuse, and narcotic abuse all produce tolerance and physical dependence over time, and withdrawal symptoms after sudden discontinuation.
This post includes material from WebMD Medical Reference.
SOURCES:
Van den Brink, W. Canadian Journal of Psychiatry, 2006.
WebMD Medical Reference: "Narcotic Abuse."
Bateson, A.N. Current Pharmaceutical Design, January 2002.
eMedicine.com: "Toxicity, Barbiturate."
Reviewed by Arefa Cassoobhoy, MD, MPH on August 01, 2013
Science on Will and Willpower - Part I
We are the only sentient creatures having the capacity to know our own will and assert our will. Frankfurt also observes, in his elegant essays, that human beings are uniquely capable of knowing that there are times when "the will that I have is not the will that I want to have." For example, someone may want to learn to play the piano, but they may say, "I can't find the will to practice." They want to have the will to practice, but somehow it's not there, or it's subordinated to a different expression of will. The same is often true of addicts and alcoholics. Wanting to stay sober, the alcoholic/addict yearns for "the will to stay sober," but often the search for the will comes up empty. Alcoholics Anonymous teaches that alcoholics cannot will themselves to quit drinking—indeed, that self-will and self-centeredness are likely a root cause of the drinking. Yet recovering addicts must be willing. That is, they must be open to the possibility that the group and its principles are powerful enough to trump a compulsive disease.
For decades Frankfurt's scholarship failed to receive the attention it deserved, and then neuroscience became an unexpected ally in the philosophical inquiry. At the University of Illinois, for example, Dr. Ibrahim Senay has studied the concepts of will and willingness from the perspective of clinical psychology. Senay figured out an intriguing way to explore possible connections among will, willingness, intention, motivation and goal-directed actions. In short, he identified some key traits needed to achieve any personal objective, from losing weight to learning to play play piano.
Senay did this by exploring self-talk. Self-talk is just what it sounds like—that voice in your head that articulates what you are thinking, spelling out your options and intentions and hopes and fears, and so forth. It is the ongoing conversation you have with yourself. Senay thought that the form and texture of self-talk—right down to the sentence structure—might be important in shaping plans and actions. What’s more, self-talk might be a tool for exerting the will—or experiencing willingness.
Senay's study involved two groups. One of the groups was told that they might be working on a task (solving a puzzle), and the other group was told that they actually would be working on a task. The first group was instructed to think about whether they would, or would not, be asked to work the puzzles. The second group was told that in a few minutes they would definitely be doing the puzzles. In this clever way, Senay created one group contemplating the question, "Will I be doing this?", and another group thinking, "I will be doing this," declaring their objective to themselves.
As it turned out, people with wondering minds (contemplating what might possibly happen) completed significantly more puzzles than did those with willful minds (thinking what they definitely were about to do). In other words, the people who kept their minds open were more goal-directed and more motivated than those who declared their objective to themselves.
The point is that questions, by their nature, speak to possibility and freedom of choice. Meditating on them might enhance feelings of autonomy and intrinsic motivation, creating a mind-set that promotes success. There is a scientifically verifiable difference between asking, and contemplating, the question "Will I?" versus narrowing the focus to a willful, determined statement, "I will."
What’s more, when the volunteers were questioned about why they felt they would be newly motivated to get to the gym more often, those primed with the question said things like: “Because I want to take more responsibility for my own health.” Those primed with “I will” offered strikingly different explanations, such as: “Because I would feel guilty or ashamed of myself if I did not.”
According to Wray Herbert, who summarized the research in Scientific American magazine, "This last finding is crucial. It indicates that those with questioning minds were more intrinsically motivated to change. They were looking for a positive inspiration from within, rather than attempting to hold themselves to a rigid standard." And there was more: "Those asserting will lacked this internal inspiration, which explains in part their weak commitment to future change. Put in terms of addiction recovery and self-improvement in general, those who were asserting their willpower were in effect closing their minds and narrowing their view of their future. Those who were questioning and wondering were open-minded—and therefore willing to see new possibilities for the days ahead."
In terms of Professor Frankfurt's metaphysical philosophy, the individual who thinks about his will and asks, "Will I?" opens the door to possibility and freedom of choice. The key to satisfaction, Frankfurt says, is "taking ourselves seriously, and getting it right."
In terms of Alcoholics Anonymous, the person who seeks to exercise willpower and "an iron will with grim determination" is much less likely to succeed. The person who struggles with AA is the person who says, "I know what I need to do, and now I just need to do it." The more successful person asks, "If I knew what I need to do, I probably would have done it by now, so I wonder what I will do?"
Do 12-Step Programs Work?
Since the 1930's when Bill W. and Dr. Bob started Alcoholics Anonymous (AA) the fellowship has grown to over two million members. Meeting in rented rooms, school halls, hospitals, and the storied church basement, AA and similar 12-step organizations (eg, Narcotics Anonymous [NA]) remain the most commonly sought sources of help for substance-related problems in the United States (Substance Abuse and Mental Health Services Administration. Results from the 2007 National Survey on Drug Use and Health: National Findings. Rockville, MD: Office of Applied Studies; 2008).
Research has shown that attending AA, either alone or during and following professional treatment, enhances outcomes. One naturalistic study, for example, followed 466 previously untreated individuals with problem drinking for eight years. Participants self-selected into one of four groups: no treatment, AA alone, formal treatment alone, and formal treatment plus AA. Those who received some sort of help—AA, formal treatment, or both—had higher rates of abstinence at all time points. At eight years, 26% of patients in the no treatment group were abstinent from alcohol compared to 49% who received AA alone, 46% who received formal treatment alone, and 58% who received the combination of treatment plus AA (Timko C et al, J Stud Alcohol 2000;61(4):529–540).
A systematic Cochrane review of the best scientific studies on AA and TSF found that they were as effective as any of the interventions to which they were compared for some factors, such as retention in treatment, but found that no studies unequivocally proved AA and TSF were superior to other treatments (Ferri M et al, Cochrane Database Syst Rev 2006;(3):CD005032).
Other studies have found a linear dose-response relationship between AA attendance and favorable drinking outcomes (Kaskutas LA, J Addict Dis 2009;28(2):145–157). Attending one meeting per week, on average, appears to be the minimum threshold to realize benefit and increasing meeting frequency is associated with progressively greater rates of abstinence. In addition, research has shown that women engage with AA as much as men, become more involved with the 12 Steps, and derive similar benefit. In 1990, the Institute of Medicine called for more research on how AA works. Since then, research has revealed that AA aids recovery through multiple mechanisms, many of which are also activated by professional behavioral treatments (Kelly J et al, Addict Res Theory 2009:17(3):236–259).
Most consistently and strongly, AA appears to work by helping people make positive changes in their social networks (eg, by dropping heavy drinkers/drug users and increasing abstainers/low risk drinkers), and by enhancing coping skills and self-efficacy for abstinence when encountering high-risk social situations (see for example, Kelly JF et al, Drug Alcohol Depend 2011;114(2–3):119–126).
Among more severely addicted people, AA also appears to work by enhancing spiritual practices, reducing depression, and increasing individuals’ confidence in their ability to cope with negative emotion (Kelly JF et al, Addiction 2012;107(2)289–299). Thus, AA appears to work through diverse mechanisms and may work differently for different people. Stated another way: individuals may use AA differently, depending on their unique needs and challenges.
Research has shown that involvement in 12-step work can reduce the need for more costly treatments while simultaneously improving outcomes. A large multicenter study of over 1,700 patients found those treated in professional 12-step treatment went on to participate in community-based AA and NA meetings at a higher rate than those from professional cognitive behavioral therapy (CBT) programs, who relied more heavily on professional services. This translated into a two-year savings of over $8,000 per patient among 12-step treated patients, without compromising outcomes. In fact, those treated in the 12-step treatment programs had one-third higher rates of abstinence across follow-up (Humphreys K & Moos R, Clin Exp Res 2001;25(5):711–716; Humphreys & Moos, Alcohol Clin Exp Res 2007;31(1):64–68).
Project MATCH was a large randomized trial comparing three individually-delivered psychosocial treatments for alcohol use disorder—TSF, CBT, and Motivational Enhancement Therapy (MET)—that was funded by NIAAA. It included 1,726 patients from nine clinical sites across the US (Project Match Research Group, J Stud Alcohol 1997;58(1):7–29). TSF was found to be as effective as the more empirically supported CBT and MET interventions at reducing the quantity and frequency of alcohol use post-treatment and at one- and three-year follow-ups. Moreover, TSF was superior to CBT and MET at increasing rates of continuous abstinence, such that 24 percent of the outpatients in the TSF condition were continuously abstinent at one year after treatment, compared with 15 percent and 14 percent in CBT and MET, respectively (Tonigan JS et al,Participation and involvement in Alcoholics Anonymous. In: Babor TF & Del Boca FK, eds. Treatment Matching in Alcoholism. New York: Cambridge University Press;2003:184–204).
Abstinence rates at three years continued to favor TSF, with 36 percet reporting complete abstinence, compared with 24 percent in CBT, and 27 percent in MET (Cooney N et al. Clinical and scientific implications of Project MATCH. In: Babor TF & Del Boca FK, eds. Treatment Matching in Alcoholism. New York: Cambridge University Press; 2003:222–237).
In light of findings from several such RCTs that demonstrated the efficacy of TSF, this therapy was added to the Substance Abuse and Mental Health Services Administration’s (SAMHSA) National Registry of Evidence-Based Practices and Programs (NREPP) in 2008.
The overwhelming majority of research has been conducted on AA. More research is needed on other MHOs, such as SMART Recovery, LifeRing, Celebrate Recovery, Women for Sobriety, Moderation Management, and others, so that more objective evidence is gathered on secular, religious, and non-abstinence-based AA alternatives (see the article "Alternatives to 12-Step Recovery" for more on these groups).
Identifying the Effective Psychiatrist
Practicing medicine is a privilege granted to very few individuals, and I am indeed fortunate. Within the field of medicine, working in psychiatry requires more than an understanding of anatomy and organ systems, because psychiatry is about the mind, the brain, the self, and human experience.
Like any other professional, I believe in high ethical standards, sound knowledge of my field, and the importance of practicing wisely and compassionately. Beyond the obvious nostrums and philosophical cliches, however, I want to be one of the good psychiatrists. As I thought about this lately, I began to wonder: how does one identify and recognize a really good psychiatrist? What makes a good psychiatrist? If I made a list of the most important aspects of a psychiatrist’s professional philosophy, what would that look like?
In 2006 an article was published in the Journal of Affective Disorders showing that good psychiatrists prescribing placebos (sugar pills) had better results than poor psychiatrists prescribing actual medication. Over 120 patients were divided into two groups, one group that received sugar pills and another group that received full strength psychiatric medication for depression. At the same time, each psychiatrist was rated on a number personal qualities: verbal fluency, interpersonal perception, expressiveness, warmth, acceptance, empathy, and the ability to focus on the other person. When results were analyzed, the psychiatrists strong in these personal qualities had the best results, even when the “medication” they prescribed was not medication at all.
The effective psychiatrists were fluent, clear, and expressive in speaking, and they had an accurate feel for their patients. Rather than being distant and aloof, the good psychiatrists were warm, friendly, and accepting. The good psychiatrists empathized well, spent more time with their patients, were more thoughtful in their strategies, and formed strong therapeutic partnerships. The point of the study was that having a good psychiatrist makes a difference in recovery.
Although medication can be extremely helpful in psychiatric care, treatment is not all about medication. The combination of the right medication, the right psychotherapy, and the right psychiatrist is the key to success.
Research has shown for generations that some clinicians consistently produce better results than others, regardless of the type of psychotherapy or theoretical orientation of the practitioner. Hundreds of studies have shown that the differences between types of psychotherapy is very small, but the psychiatrist providing the psychotherapy is critically important.
Over the past fifteen years, extensive research has given us a solid body of evidence about the qualities and actions of effective psychiatrists. Based on the psychotherapy research of Dr. Bruce Wampold of The University of Wisconsin, I have formulated here an inventory that provides the basis for judging whether a psychiatrist is likely to be effective.
- Effective psychiatrists demonstrate a sophisticated set of interpersonal skills, including verbal fluency, perceptiveness of others, emotional intelligence, expressiveness, warmth, and acceptance. Given these gifts, the most effective psychiatrists are those who are first excellent physicians, well trained in medicine, competent to practice at the highest levels.
- Effective psychiatrists are inquisitive, questioning, and seeking new knowledge constantly. They embrace science while at the same time possessing the humility to know how little we really know.
- Patients of effective psychiatrists feel understood, trust the psychiatrist, and believe the psychiatrist can help. The psychiatrist creates these conditions in the first moments in both speech and action. In the initial contacts, patients are very sensitive to cues of acceptance, understanding, and expertise. Although these conditions are necessary throughout therapy, they are most critical in the initial interaction to ensure engagement in the therapeutic process.
- Effective psychiatrists are able to form a working alliance with a broad range of patients. The working alliance involves the therapeutic bond, but also importantly agreement about the task of goals of therapy. The working alliance is described as collaborative, purposeful work on the part of the patient and the psychiatrist. The effective psychiatrist builds on the patient’s initial trust and belief to form this alliance and the alliance becomes solidly established early in therapy.
- Effective psychiatrists provide an acceptable and practical explanation for the patient’s distress. The patient wants an explanation for his or her symptoms or problems. There are several considerations involved in providing the explanation. First, the explanation must be consistent with the healing practice. On the medical side, the explanation is biological, and in psychotherapy the explanation is psychological. Second, the explanation must be acceptable and compatible with the patient’s attitudes, values, culture, and worldview. Third, the explanation must provide a strategy by which the patient can overcome difficulties and solve life’s problems. These three factors together make for a strong therapeutic alliance.
- The effective psychiatrist provides a treatment plan that is consistent with the explanation provided to the patient. Once the patient accepts the explanation, the treatment plan will make sense and patient compliance will be increased. The treatment plan must involve healthy actions—the effective psychiatrist promotes healing by replacing failed strategies with effective strategies. At the same time, strong defenses will replace weak defenses, and healthy practices will replace self-defeating behaviors.
- The effective psychiatrist is influential, persuasive, and convincing. The psychiatrist presents the explanation and the treatment plan in a way that convinces the patient that the explanation is correct and that following through with the treatment will benefit the patient. This process leads to patient hopefulness, increased expectancy for mastery, and healthy actions. These characteristics are essential for forming a strong working alliance.
- The effective psychiatrist is honest and authentic. Authenticity refers to communication to the patient that the psychiatrist truly wants to know how the patient is doing. The best psychiatrists tend not to use checklists, scales, and paper measures. Instead, they talk and listen openly and honestly.
- The effective psychiatrist is flexible and will be patient if resistance to the treatment is apparent or the patient is slow to make progress. Although the effective psychiatrist is persuasive, persuasion can be a process that takes time. The good psychiatrist pays attention, takes in new information, test hypotheses about the patient, and is willing to be wrong. A good psychiatrist will seek second opinions, refer to other specialists, and even take calculated risks such as trying a new approach or a newly released medication.
- The effective psychiatrist does not avoid difficult material in therapy. Doctor and patient must use such difficulties therapeutically. We all tend to avoid material that is difficult. The effective psychiatrist senses avoidance is taking place and does not collude to avoid the material. Instead, the psychiatrist will discuss the difficult material and address difficult problems. Sometimes conversations can be difficult, and at times the relationship between doctor and patient can be strained, but this is part of the work of therapy. The good psychiatrist can use skill, experience, and compassion to overcome these barriers to recovery.
- The effective psychiatrist communicates hope and optimism. Sometimes this is easy to do, and sometimes it’s difficult. The working partnership must maintain hope and optimism in the face of chronic illness, relapses, lack of consistent progress, and many other difficulties. Effective psychiatrists acknowledge these issues and still communicate hope that the patient will achieve realistic goals in the long run. This communication is not blind faith or Pollyanna optimism, but rather a firm belief that together the psychiatrist and patient will work successfully. At the same time, effective psychiatrists mobilize patient strengths and resources to facilitate the patient’s ability to solve his or her own problems. The best doctors know that the patient, through his or her work, is responsible for therapeutic progress, creating a sense of mastery.
- Effective psychiatrists are aware of the patient’s characteristics and context. This is a tall order with many categories: culture, race, ethnicity, spirituality, sexual orientation, age, physical health, motivation for change, and beyond. Furthermore, the effective psychiatrist is aware of how his own background, personality, and beliefs figure into the relationship.
- The effective psychiatrist is aware of his or her own psychological process and does not inject his or her own material into the therapy process unless such actions are deliberate and therapeutic.
- The effective psychiatrist is aware of the best research evidence related to the particular patient, in terms of treatment, problems, and social context. It is very important to understand the biological, social, and psychological basis of the patient’s problem.
- The effective psychiatrist seeks always to improve, always to be a student. Hippocrates said, “The life so short, the craft so long to learn,” and truer words were never spoken.
- Finally, the good psychiatrist must possess both humility and a sense of humor. We will never know enough, or be wise enough, to have all the answers. We cannot take ourselves too seriously, lest we become arrogant, prideful, and set ourselves apart from those who have graced us with the privilege of being socially sanctioned healers.
Development of skill in psychiatry involves intensive practice and unceasing professional growth. Patients are sometimes our best and most effective teachers. A few years ago I taught a seminar for third year students at the University of Texas Southwestern Medical School, “Psychiatric Nightmares, Disasters, and Catastrophes.” The entire content of the seminar consisted of mistakes I’d made, errors I had committed, and pitfalls that these students likely would encounter, sooner or later, in their medical careers.
I told the story of a patient with whom I’d had a terrible, angry argument, and how guilty I felt for years about my lack of composure—only to have the patient return, two years later, to ask me for a job at the hospital and tell me that she had been shaken into reality by our confrontation. I told them the story of the patient who overdosed and came to the ICU, and how I was baffled by the case—until I realized that the patient had diabetes, and was actually in a diabetic coma, not a drug-induced state.
I told them about the patient who came to the doorstep of my home on a Sunday afternoon, bearing in her arms her injured pet cat, hoping that I could help. I told them about an elderly man from New Orleans who was my patient in the middle of the night as Hurricane Katrina washed away his home.
And I told them about the time when I was called to the ER to examine a beautiful young woman, a Duke University cheerleader, who had bruised her shoulder. When I approached her to examine the injury, and she undid her gown and dropped it with a smile, I calmly reached into the pocket of my white coat for my stethoscope, only to realize that I then stuck my reflex hammer in my ear.
These encounters are the building blocks of the effective psychiatrist’s life. I’ve come to realize that most of the learning happens after we graduate. As Dr. Stead used to say at Duke, “Medical school is where you stay for four years until you’re old enough to become a doctor.”
Neuroscience of Belief
In 1921, philosopher Bertrand Russell put it succinctly when he described belief as "the central problem in the analysis of mind". Believing, he said, is "the most 'mental' thing we do" – by which he meant the most removed from the "mere matter" that our brains are made of. How can a physical object like a human brain believe things? Philosophy has made little progress on Russell's central problem. But increasingly, scientists are stepping in.
The neuroscientific investigation of belief began in 2008, when Sam Harris (Harris, S., Sheth, S. A. and Cohen, M. S. (2008), Functional neuroimaging of belief, disbelief, and uncertainty. Ann Neurol., 63: 141–147) at the University of California, Los Angeles, put people into a brain scanner and asked them whether they believed in various written statements. Some were simple factual propositions, such as "California is larger than Rhode Island"; others were matters of personal belief, such as "There is probably no God". Harris found that statements people believed to be true produced little characteristic brain activity – just a few brief flickers in regions associated with reasoning and emotional reward. In contrast, disbelief produced longer and stronger activation in regions associated with deliberation and decision-making, as if the brain had to work harder to reach a state of disbelief. Statements the volunteers did not believe also activated regions associated with emotion, but in this case pain and disgust.
To read the full article, click here.
Two Talks Today to Good Teams
Be a Better Spouse or Partner
#1 Be nice as often as you can.
A lot of modern relationship therapy is based on the research of John Gottman, a prolific psychologist famous for videotaping thousands of couples and dissecting their interactions into quantifiable data. One of his most concrete findings was that happier couples had a ratio of five positive interactions to every negative interaction. “That just leapt off the pages of the data analysis,” he says. It was true in very different types of relationships, including those in which the people were very independent and even distant or argumentative. These positive interactions don't have to be grand gestures: “A smile, a head nod, even just grunting to show you're listening to your partner—those are all positive,” Gottman says.
#2 Think about what your partner needs, even when fighting.
To resolve conflicts, Gottman says we can learn from game theory—the study of conflict and decision making used in political science, sociology and economics. It used to be widely accepted that negotiations were mostly zero-sum situations, meaning one party's gain was the other party's loss. In 1950 mathematician John Nash proved there was another, better outcome: a solution in which the parties may have to compromise, but in the end all of them come out satisfied. (This now famous “Nash equilibrium” won him a Nobel Prize in 1994.) I'm reminded of a recent situation in my own marriage—my husband hated the house we bought a couple of years ago and wanted to move to a different neighborhood; I liked the house just fine and didn't want to goanywhere. After much discussion, we realized that what we both really want is to settle in somewhere for the long haul. If the current house is not a place my husband feels he can settle in, then I can't truly settle in either. So we're moving next month, for both our sakes! Find the Nash equilibrium in your conflict, and you'll both get your needs met.
#3 Just notice them.
“People are always making attempts to get their partners' attention and interest,” Gottman says. In his research, he has found that couples who stay happy (at least during the first seven years) pick up on these cues for attention and give it 86 percent of the time. Pairs who ended up divorced did so 33 percent of the time. “It's the moment we choose to listen to our partner vent about a bad day instead of returning to our television show,” explains Dana R. Baerger, assistant professor of clinical psychiatry and behavioral sciences at the Northwestern University Feinberg School of Medicine. “In any interaction, we have the opportunity to connect with our partner or to turn away. If we consistently turn away, then over time the foundation of the marriage can slowly erode, even in the absence of overt conflict.”
#4 Ignore the bad, praise the good.
Observations of couples at home reveal that people who focus on the negative miss many of the positive things that their partners are doing. Happy spouses, however, ignore the annoyances and focus on the good. “If your wife is irritable one morning, it's not a big deal. It's not going to become a confrontation,” Gottman says. “Then when she does something nice, you notice and comment on that.” Guess what that breeds? More of the good stuff.
Public Speaking & Talks
I've also included a list of topics from my speaking schedule over the past few years. I've noted the talks that got the highest reviews, which means that at least 90% of the reviews were 4 or better on a 5 point scale. Some talks did not include feedback, but the topics listed here have all been well received.
If your organization would like to schedule a talk, lecture, or workshop, give me a call. As my schedule permits, I am happy to speak for churches, schools, parent groups, and not-for-profit organizations at no charge.
New in 2015!
Four Sides to Every Story: Understanding and Helping the Whole Patient (highly rated)
Mindfulness: An Essential Practice in Recovery from Alcohol and Drugs
Beyond Motivation: The Positive Psychology of Excellent Addiction Treatment
Beyond the Basics: The Advanced Course in 12 Step Recovery
When Therapy Fails: Troubleshooting and Solutions
Mental Health Topics
Stress, Depression, and Burn-out (highly rated)
The Problems of Anxiety and Depression
What is Bipolar Disorder?
Chronic Mental Illness and the Seriously Mentally Ill
Attention Deficit Disorder: Causes, Concerns, and Cures
Alcohol and the Family (highly rated)
PTSD: Myths and Realities
Gambling: Deadly Odds and Destructive Desires
Street Drugs: The Facts
Addictions and the Future of Theory and Practice
Veterans and the VA: Hard Times for Mental Health (highly rated)
Family Topics
Scientific Evidence About Happy Marriages (highly rated)
Keys to Happier Relationships (highly rated)
ADD: What Parents Need to Know (highly rated)
Talking With Children About Drugs and Alcohol
Oppositional Children and Difficult Behavior (highly rated)
Marriage: How It Works, How It Breaks Down, How to Fix It
How My Wife Raised Three Successful Children (With My Help)
Single Mothers and Their Daughters (highly rated)
Raising Responsible Children
Families of Divorce
Yes Is a Dangerous Word (The Price of Permissiveness)
Youth Suicide: What We Know, What We Don’t Know
Learning Differences: Understanding How the Brain Is Wired
General Topics
An Introduction to Mindfulness (highly rated)
An Introduction to Positive Psychology (highly rated)
What is Personality? The Nine Types of People You Know (highly rated)
Emotional Intelligence: Hot Topic or Hot Air?
How Poker, Bridge, and Chess Prevent Alzheimer’s Disease
Why Philosophy Matters
Happiness: The Facts
A Short History of Psychology and Psychiatry
My Time on Death Row: A Huntsville Memoir
Topics in Spirituality
Why Does God Allow Suffering? (highly rated)
The Importance of Spiritual Practice and Discipline (highly rated)
Why Is Prayer So Difficult?
Religion and World Problems
The Dangers of Fundamentalism (highly rated)
Belief and Reality: What’s the Difference?
Treatment Philosophy
My approach to psychiatric practice reflects many years studying human nature and working to help people who are having a hard time in life. By the time most people see a psychiatrist, they are worried, or they are sad, or they are very confused about something I will just call “the problem,” or “the complaint.” Let me make some general comments about my approach, and then I will discuss my thinking on the use of medications.

People seek psychiatric help for a variety of problems, but everyone wants the same result: to feel better, to think more clearly, to rediscover satisfaction and happiness, and to regain a sense of self control and personal freedom. The problem may be related to mood, energy level, motivation, sleep, worry, relationships, anger, troubled behavior, obsessions, compulsions -- it’s a long list. People who drink too much, use drugs, or misuse prescription medication are often using these chemicals to find relief. Alcoholism and substance abuse are widespread in our culture.
Dealing with life is never easy.
Most persons first try to solve the problem or deal with the complaint on their own. Frustrated that things aren’t improving, they may seek advice from others. Sometimes a person hides the problem or lives in silence with the complaint. They may read a book, go to a support group, consult the internet, or try a new religious practice. We all have problems and complaints, and we all do the best we can to solve the dilemmas of life. When someone calls me about consultation, I almost always hear them say that they have a problem, they have tried to solve the problem, and they are looking for someone who knows how to help make things better.
One of the individuals consulting with me said, “I feel like I’m in a box, and the directions for getting out of the box are printed -- on the outside of the box.”
A successful airline pilot, a Vietnam combat veteran, said, “Doc, I’m out of altitude, airspeed, and ideas.”
Often the person seeking help has waited so long that demoralization has begun to set in, and they are beginning to lose hope. This doesn’t mean that the individual is suicidal or, in fact, any more unhappy than many of the people at the workplace or in the neighborhood. It means that they are resigned to always feeling this way, never feeling any better than this. Demoralization means a state of mind in which a person considers accepting fate, giving up, and abandoning the idea that things can get better.
Fear, anger, resentment, feeling constantly wounded, feeling overwhelmed, feeling unappreciated, feeling worthless -- all of these emotions are part of our lives. But when we feel negative all the time, or most of the time, most days, then we need help. There are very few emotional problems that defy intelligent therapy and reasonable efforts toward a solution.
When I meet someone for the first time in consultation, I have three major concerns. First, I want to get to know the person and hear about the problem are the complaint. My first question usually is simply, “How can I help?” or “What brings you to see me?” Second, I want to explore the individual’s point of view or understanding of the problem, including what solutions have been attempted. Third, I want to consider what we can do, working together, to improve the situation. I tend to focus more on results than on reasons. I’m not always sure about why things happen, but I am very focused on what we can do now. Sometimes I explain in detail how the brain works, and sometimes I discuss how life works. The process of recovery involves growth, change, and even personal transformation.
Research shows that psychotherapy can help, medication can help, and intelligent problem solving helps. Psychotherapy is not for everyone, and medication is not for everyone, but the vast majority of people who want help can find it. One of my favorite expressions is, “You have to do it yourself, but you can’t do it alone.”
Over the years I have developed a style that I call “sober conversation.” The word “sober” does not apply just to alcohol and addictions. To be sober is to be serious, to focus on what is most important, and to try to get it right. I believe in the importance of what we care about, and in this regard I have seriously studied the specific problem of human will. I call it “the problem of human will” because we are often confused about what we will ourselves to do, or not to do. When I work as a psychotherapist, I am most interested in what people care about, how their beliefs and assumptions about life have been formed, and where they feel stuck or at odds with themselves. Sometimes we have conflicting feelings about the same thing. For example, someone wants to take life in a certain direction, but he or she feels conflicted about it. Or someone tries to solve a problem, not realizing that it’s part of a bigger problem, or a different kind of problem. My definition of psychotherapy is that it is a form of personal consultation, focused on the situation of the client, with the goal of solving problems and feeling better.

Not everyone is cut out for in-depth or long-term conversation. Some people like to come for a few visits, and some like to keep going for weeks, or even months on a weekly basis. Some people prefer to come two or three times a week because they want to do the work and get on with whatever is next. Some people come for an hour, and some come for an afternoon.
Psychotherapy does take time, because the process is basically two people getting to know each other in the context of a specific purpose. Psychotherapy at its best is about taking life seriously, getting it right, and feeling the satisfaction that comes from clarity of thought, commitment to integrity, and comfort with the complexity of one’s own emotions and ideas. Some say that psychotherapy is a dying art, and this may be true. Psychiatrists today (and perhaps psychologists as well) do not receive the extensive training in psychotherapy that we did thirty years ago. Many psychiatrists and psychologists are not interested in psychotherapy. And many psychotherapists are not really very good or very well trained. Today there are thousands of people who call themselves “life coaches,” and anyone can hang out a shingle and call himself a “life coach.” There are several private organizations that offer “certifications,” but there are no license requirements, there is no government regulation, and no educational standard that is generally accepted. For these reasons, I think the concept makes sense, but in practice let the buyer beware -- caveat emptor!
Medications can be very helpful in treating some specific psychiatric problems. Today we have excellent medications for anxiety, depression, moodswings, insomnia, attention deficit disorder, and other conditions. Bipolar disorder, for example, is a devastating condition that can be very effectively managed with medication, restoring individuals to a life of normalcy and stability. I have absolutely no doubt about the value of psychiatric medications. I also believe that what is most important is getting the right diagnosis and the correct strategy for intervention and treatment. I see many people who have been misdiagnosed, and even mistreated, because they have not been well assessed. Assessment can take time, and I never jump to conclusions about diagnosis. After knowing someone for a few weeks, together we may decide that we see the condition in a different way.
Psychiatric medications are powerful, effective tools when used properly, but they also have side-effects, and they are expensive. Getting the right medication for the right diagnosis is extremely important. And there is an old saying from Hippocrates, creator of The Hippocratic Oath: “It is more important to know what sort of person has a disease than to know what sort of disease a person has.“
Thoughts and Reflections
Psychiatry as a medical specialty is a vast—and often uncharted—territory. The basic education of a psychiatrist is highly scientific and technical. The first two years of medical school are purely basic science: anatomy, physiology, biochemistry, microbiology, and so on. The last two years include brief exposure to psychiatry and psychology, but most of the time is devoted to medicine, surgery, ob-gyn, and pediatrics. Internship and residency years in psychiatry involve patient care, but the psychiatrist’s true education begins after graduation. As the venerable Dr. Eugene Stead used to tell us at Duke, “Medical school is where you stay until you’re old enough to learn how to be a doctor.” The education of the good psychiatrist is a process that lasts a lifetime.
Thanks for reading!