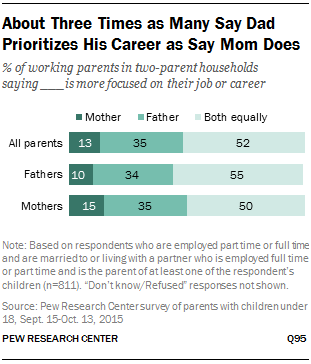
Families, Pressure, & Stress
Working mothers (60%) are somewhat more likely than fathers (52%) to say it’s difficult for them to balance work and family, and this is particularly the case for mothers who work full time. In fact, one-in-five full-time working moms say balancing the two is very difficult for them, compared with 12% of dads who work full time and 11% of moms who work part time.
Overall, relatively few working parents (9%) say parenting is stressful for them all of the time. But a significant share say that parenting is stressful all or most of the time, and that sentiment is much more common among parents who say they have difficulty balancing work and family life (32% compared with 15% of those who say achieving a work-life balance is not difficult for them). In addition, four-in-ten (39%) of those who say it is hard for them to balance their responsibilities at work and at home find being a parent tiring at least most of the time; of those who say it’s not difficult for them to strike a balance, 23% say being a parent is tiring at least most of the time.
Fifty-six percent of all working parents say the balancing act is difficult, and those who do are more likely to say that parenting is tiring and stressful, and less likely to find it always enjoyable and rewarding. For example, half of those who said the work-family balance was not difficult said parenting was enjoyable all the time, compared with 36 percent of those who said balance was difficult.
In her 1989 book The Second Shift, the sociologist Arlie Russell Hochschild described the double burden employed mothers face because they are also responsible for housework and child care. Last year she said that despite some changes in society, the workplace had not changed enough to alleviate the problems. In another widely praised book, All Joy and No Fun, the journalist Jennifer Senior described how little had improved: Working parents face similar stresses, but they are now exacerbated by the expectations of modern parenthood and shared by fathers, too.
Senior draws on the psychologist Daniel Kahneman’s distinction between the “experiencing self” that exists in the present moment and the “remembering self” that constructs a life’s narrative. “Our experiencing selves tell researchers that we prefer doing the dishes — or napping, or shopping, or answering emails — to spending time with our kids. But our remembering selves tell researchers that no one — and nothing — provides us with so much joy as our children. It may not be the happiness we live day to day, but it’s the happiness we think about, the happiness we summon and remember, the stuff that makes up our life-tales.” She talks about parents’ pride in their children, not only in their accomplishments but even in their basic development as human beings, their growth into kindness and generosity. “Kids may complicate our lives,” she writes. “But they also make them simpler. Children’s needs are so overwhelming, and their dependence on us so absolute, that it’s impossible to misread our moral obligation to them. We bind ourselves to those who need us most, and through caring for them, grow to love them, grow to delight in them, grow to marvel at who they are.”
Those Danged Cognitive Distortions
1. ALL-OR-NOTHING THINKING: You see things in black-and-white categories. If performance falls short of perfect, you see yourself or others as total failures.
2. OVERGENERALIZATION: You see a single negative event as a never-ending pattern of defeat. Phrases like "You always …" or "You never …" exemplify overgeneralization.
3. MENTAL FILTER: You pick out a single negative detail and obsess on it so that your vision of all reality becomes darkened, like the drop of ink that discolors an entire glass of water.
4. DISQUALIFYING THE POSITIVE: You reject positive experiences by insisting they "don't count" for some reason or other. In this way you can maintain a negative belief that is contradicted by your everyday experiences. Often this manifests as making excuses when somebody pays you a compliment.
5. JUMPING TO CONCLUSIONS: You make a negative interpretation even though there are no definite facts that convincingly support your conclusion often a "wait and see" attitude is called for in these situations.
• MIND READING: You arbitrarily conclude (usually by personalizing their behavior) that someone is reacting negatively to you, and you don't bother to check this out.
• THE FORTUNE TELLER ERROR: You often anticipate that things will turn out badly, and you feel convinced that your prediction is an already-established fact.
6. MAGNIFICATION (CATASTROPHIZING) OR MINIMIZATION: You exaggerate the importance of things (such as your achievements or someone else's goof up), or you inappropriately shrink things until they appear tiny (your own character defects or other people's acceptable behavior). This is also called the "binocular trick."
7. EMOTIONAL REASONING: You allow your negative emotions to color how you see the world with an "I feel it, therefore it must be true."
8. SHOULD STATEMENTS: You try to motivate yourself or others with should and shouldn't, as if needing be whipped and punished before you could be expected anything. "Musts" and "oughts" are also offenders. The emotional consequences are guilt. When you
direct should statements toward others, you feel anger, frustration, and resentment as do they!
9. LABELING AND MISLABELING: This is an extreme form of overgeneralization. Instead of describing your error, you attach a negative label to yourself. "I'm a loser." When someone else's behavior rubs you the wrong way, you attach a negative label to him "He's a dumb jerk!" Mislabeling involves describing an event with language that is highly colored and
emotionally loaded, and generally not factually descriptive.
10. PERSONALIZATION: You see yourself as the cause of some negative external event, which in fact you were not primarily responsible for.
My generation of psychiatrists was the first to break with the old-fashioned, unscientific model known as Freudian psychoanalysis—the stereotype of the patient lying on the couch for years and being "analyzed" by the shrink. For some reason, our generation just didn't see this as very helpful or useful. Psychoanalysis in its pure form means 4-5 visits a week to the psychoanalyst, and the typical course of therapy is measured in years! There were no outcome studies proving the effectiveness of this approach. We really wanted something that would produce results, and an approach that the average person could afford.
Dr. Ben Martin at PsychCentral describes the new, scientific talk therapy this way: Cognitive behavioral therapy (also known by its abbreviation, CBT) is a short-term, goal-oriented psychotherapy treatment that takes a hands-on, practical approach to problem-solving. Its goal is to change patterns of thinking or behavior that are behind people’s difficulties, and so change the way they feel. It is used to help treat a wide range of issues in a person’s life, from sleeping difficulties or relationship problems, to drug and alcohol abuse or anxiety and depression. CBT works by changing people’s attitudes and their behavior by focusing on the thoughts, images, beliefs and attitudes that we hold (our cognitive processes) and how this relates to the way we behave, as a way of dealing with emotional problems.
An important advantage of cognitive behavioral therapy is that it tends to be short, taking four to seven months for most emotional problems. Clients attend one session per week, each session lasting approximately 50 minutes. During this time, the client and therapist are working together to understand what the problems are and to develop a new strategy for tackling them. CBT introduces them to a set of principles that they can apply whenever they need to, and which will stand them in good stead throughout their lives.
Cognitive behavioral therapy can be thought of as a combination of psychotherapy and behavioral therapy. Psychotherapy emphasizes the importance of the personal meaning we place on things and how thinking patterns begin in childhood. Behavioral therapy pays close attention to the relationship between our problems, our behavior and our thoughts.
SMART Training for Teens
Teen SMART Camp is a great chance for your children or grandchildren to boost their frontal lobe functioning and gain important strategies for learning.
For questions and registration, please contact Lindsay Gehan at Lindsay.Gehan@utdallas.edu or 972.883.3310
Over the last six years, BrainHealth researchers have trained more than 27,000 students in SMART through research grants. Results have shown significant changes in frontal lobe regions responsible for higher order thinking and problem solving after only 10 hours of training. SMART has shown substantial improvements in academic performance in those who have participated to date.
SMART is a series of seven cognitive strategies that can be applied to any learning context. As students’ progress through these steps, they learn to discard unsuccessful and superficial learning styles and to adopt a more robust, focused, and deeper-level strategic learning approach. Upon completion of the SMART training, students can apply the methodology to any subject and have been shown scientifically to do so over an extended period of time with success.
This summer’s teens will begin SMART Camp by receiving comprehensive strategy instruction, teaching them to use their brains more efficiently to improve learning. SMART campers employ their new strategies in a variety of fun learning activities involving academic content as well as personally-relevant materials such as their favorite song lyrics, television shows, magazine articles, or movies, emphasizing organizational and motivational skills. The training is designed to help the teens apply their newly learned strategies to everyday situations. Each camper works on an individual and a group project over the course of the camp to practice planning, goal setting and time management.
The brain is primed for higher order reasoning beginning in adolescence. As a result, this SMART program is offered for students who will enter the 7th through 12th grade in Fall 2015.
SMART Camp has a maximum enrollment of 20 students and are filled on a first-come, first serve basis. The full payment amount is due before the camp begins.
Schedule:
June 22-26th 2015 – The day will start promptly at 9:00 am and conclude at 3:00 pm.
SMART Camp takes place over one week at the Center for BrainHealth.
Please contact Lindsay Gehan at Lindsay.Gehan@utdallas.edu or 972-883-3310 for more information
Science on Will and Willpower - Part II
An excellent video of one of Roy's lectures is on my media page.
We try to control ourselves in all sorts of ways: eating right, exercising, avoiding drugs and alcohol, studying more, working harder, spending less. Baumeister says that the practical significance of all this is enormous. He says: "Most of the problems that plague modern individuals in our society — addiction, overeating, crime, domestic violence, sexually transmitted diseases, prejudice, debt, unwanted pregnancy, educational failure, underperformance at school and work, lack of savings, failure to exercise — have some degree of self control failure as a central aspect."
Baumeister goes on to say that two main traits that seem to produce an immensely broad range of benefits: intelligence and self-control. However, psychology has not found much one can do to produce lasting increases in intelligence. On the other hand, self-control can be strengthened, and the study of self-control is a rare and powerful opportunity for psychology to make a palpable and highly beneficial difference in the lives of ordinary people.
For example, in his research he has found that people perform relatively poorly on tests of self-control when they have engaged in a previous, seemingly unrelated act of self-control: "For instance, in a study in my lab, we invited some students to eat fresh-baked chocolate-chip cookies, and asked others to resist the cookies and munch on radishes instead. Then we gave them impossible geometry puzzles to solve. The students who ate the cookies worked on the puzzles for 20 minutes, on average. But the students who had resisted the tempting cookies gave up after an average of eight minutes."
"Such studies suggest," he continues, "that some willpower was used up by the first task, leaving less for the second. The pattern is opposite to what one would expect based on priming or activating a response mode. So we began to think that some kind of limited resource is at work: It gets depleted as people perform various acts of self-control. Over time, we have begun to link this resource to the folk notion of willpower."
Making decisions seems to use up our willpower. After making decisions, people perform worse at self-control. Conversely, after exerting self-control, decision-making shifts toward simpler and easier processes. That can lead people to make poorer decisions, or to avoid making choices at all. Apparently, decision making depletes the same resource as self-control.
One of Baumeister's examples of willpower depletion: "A dieter may easily avoid a doughnut for breakfast, but after a long day of making difficult decisions at work, he has a much harder time resisting that piece of cake for dessert. Another example might be losing your temper. Normally, you refrain from responding negatively to unpleasant things your romantic partner says. But if one day you’re especially depleted — maybe you’re trying to meet a stressful work deadline — and the person says precisely the wrong thing, you erupt and say the words you would have stifled if your self-control strength was at full capacity. What do you call this process? My collaborators and I use the term “ego depletion” to refer to the state of depleted willpower. Initially, we called it “regulatory depletion” because the first findings focused purely on acts of self-regulation. When it emerged that the same resource was also used for decision-making, we wanted a broader term that would suggest some core aspect of the self was depleted. We borrowed the term “ego” from Freudian theory because Freud had spoken about the self as being partly composed of energy and of processes involving energy."
In his book, Baumeister explains that some people imagine that self-control or willpower is something you only use once in a while, such as when you are tempted to do something wrong. The opposite is true. Research indicates that the average person spends three to four hours a day resisting desires. Self-control is used for other things as well: controlling thoughts and emotions, regulating task performance and making decisions. Most people use their willpower many times a day, all day. And toward the end of the day, there is less gas in the tank.
We now know that people can improve their self-control even as adults. As with a muscle, it gets stronger from regular exercise. So engaging in some extra self-control activities for a couple weeks produces improvement in self-control, even on tasks that have no relation to the exercise activities. The exercises can be arbitrary, such as using your left hand instead of your right hand to open doors and brush your teeth. Or they can be meaningful, such as working to manage money better and save more. The important thing is to practice overriding habitual ways of doing things and exerting deliberate control over your actions. Over time, that practice improves self-control. As people deplete willpower, they became increasingly likely to give in to desires they might otherwise have resisted. This was true for all manner of desires: desires to sleep, to eat, to have sex, to play games, to spend money, to drink alcohol or smoke cigarettes.
One of the best features of Roy Baumeister's work, particularly his book on willpower, is that he is easy to read, accessible to those of us not trained in clinical research or adept at deciphering scientific papers.
Videos Added to My Site
Genetics, Weird Facts, & Placebos
A placebo is anything that seems to be a "real" medical treatment -- but isn't. It could be a pill, a shot, or some other type of "fake" treatment. What all placebos have in common is that they do not contain an active substance meant to affect health. Younger physicians won't remember this, but years ago it was considered okay for doctors to prescribe placebos. Surgeons fairly often would substitute saline (salt water) injections when they worried that patients were asking for too many narcotic shots after an operation. There was a preparation called Gevrabon that was essentially sherry wine with some vitamins added, and it could be given by prescription "for relaxation at bedtime." Over the years, for obvious reasons, experts in medical ethics began to question whether these practices—essentially deceiving patients, but with good intentions—were proper and permissible.
In addiction medicine, I've seen college students come into the emergency room looking drunk, only to discover (with lab verification) that the "drug" they had tried was simply a vitamin pill. Similar findings have emerged at The University of Texas Austin, where one of the research labs has a full-fledged bar (i.e. a saloon) set up to simulate the settings where college students drink. Click here to see the Sahara Bar in the Department of Psychology. Study subjects sometimes get tipsy even when their margarita or manhattan contains no alcohol at all.
In 1996, scientists assembled a group of students and told them that they were going to take part in a study of a new painkiller, called "trivaricaine". Trivaricaine was a brown lotion to be painted on the skin, and smelled like a medicine. But the students were not told that, in fact, trivaricaine contained only water, iodine, and thyme oil – none of which are painkilling medicines. It was a fake – or placebo – painkiller. Read an abstract of the study: Mechanisms of Placebo Pain Reduction. With each student, the trivaricaine was painted on one index finger, and the other left untreated. In turn, each index finger was squeezed in a vice. The students reported significantly less pain in the treated finger, even though trivaricaine was a fake.
In this example, expectation and belief produced real results. The students expected the "medicine" to kill pain: and, sure enough, they experienced less pain. This is the placebo effect.
Placebo medicine has even been shown to cause stomach ulcers to heal faster than they otherwise would. These amazing results show that the placebo effect is real, and powerful. They mean that fake or placebo treatments can cause real improvements in health conditions: improvements we can see with our own eyes. Experiencing the placebo effect is not the same as being "tricked", or being foolish. The effect can happen to everyone, however intelligent, and whether they know about the placebo effect or not.
An article in Harvard Magazine describes Harvard Professor Dr.Ted Kaptchuk’s first randomized clinical drug trial, where nearly a third of his 270 subjects complained of awful side effects. All the patients had joined the study hoping to alleviate severe arm pain: carpal tunnel, tendinitis, chronic pain in the elbow, shoulder, wrist. In one part of the study, half the subjects received pain-reducing pills; the others were offered acupuncture treatments. And in both cases, people began to call in, saying they couldn’t get out of bed. The pills were making them sluggish, the needles caused swelling and redness; some patients’ pain ballooned to nightmarish levels. “The side effects were simply amazing,” Kaptchuk explains; curiously, they were exactly what patients had been warned their treatment might produce. But even more astounding, most of the other patients reported real relief, and those who received acupuncture felt even better than those on the anti-pain pill. These were exceptional findings: no one had ever proven that acupuncture worked better than painkillers. But Kaptchuk’s study didn’t prove it, either. The pills his team had given patients were actually made of cornstarch; the “acupuncture” needles were retractable shams that never pierced the skin. The study wasn’t aimed at comparing two treatments. It was designed to compare two fakes.
Dr. Kaptchuk and his colleagues have found that placebo treatments—interventions with no active drug ingredients—can stimulate real physiological responses, from changes in heart rate and blood pressure to chemical activity in the brain, in cases involving pain, depression, anxiety, fatigue, and even some symptoms of Parkinson’s. His work was also featured in a New Yorker article, "The Power of Nothing," that can be found here.
Here are four fascinating (and weird) facts about placebos and the placebo effect:
1. It doesn't have to be a secret. Some believe that a placebo can only work if the recipient is unaware they are taking one. But there's evidence that people with irritable bowel syndrome who knowingly receive a placebo do better than those who are left untreated.
2. It works better if it's expensive. The pain-killing power of a placebo pill is greater among people who are told they are taking a full-price version, compared to those told that the pill is on sale for a discounted price.
3. It's not just us, animals can get it too. A 2012 study found that between 30 and 40 per cent of rats experienced pain relief when their morphine injections were swapped for inactive saline solution.
4. It has an evil twin. The nocebo effect makes people undergoing treatment more likely to suffer from side-effects if they are warned about them by their doctor.
For the full New Scientist journal article on the subject, click here.
Slowly, over the past decade, researchers have begun to tease out the strands of the placebo response. The findings, while difficult to translate into medicine, have been compelling. In most cases, the larger the pill, the stronger the placebo effect. Two pills are better than one, and brand-name pills trump generics. Capsules are generally more effective than tablets, and injections produce a more pronounced effect than either. There is even evidence to suggest that the color of medicine influences the way one responds to it: colored pills are more likely to relieve pain than white pills; blue pills help people sleep better than red pills; and green capsules are the best bet when it comes to anxiety medication.
Being Mindful and Positive
Mindfulness is natural, but we often overlook the importance of living in the present moment. There is not much new to learn; it's more about being aware of what is happening, who we are, and how to practice. We already have the capacity to be present, and it doesn’t require us to change who we are. You will hear me describe, in our conversations, topics like attention, awareness, empathy, compassion, being in the zone, situational awareness, presence, flow, contemplation, and many more. Being mindful has the power to change how we approach ourselves, our work, our relationships, and our communities. Mindfulness practice should be part of everyone's toolbox in the process of recovery from any mental or emotional setback. On my links page I have listed some useful resources on the subject.
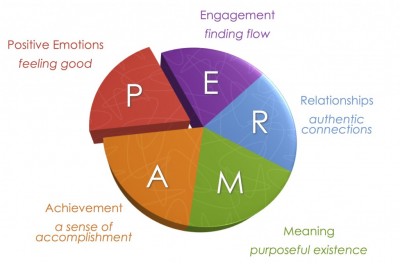
Positive psychology began to emerge in the late 1980's through the research of my colleague Dr. Martin Seligman. If you have attended my talks on the positive psychology of addiction recovery, you've heard me describe "PERMA," the five dimensions of life where positive psychology produces meaningful results. Seligman outlines the categories in his book, Authentic Happiness. The acronym for the five elements of Seligman’s well-being theory is PERMA (Positive Emotions, Engagement, Relationships, Meaning and purpose, and Accomplishments).
What people in addiction recovery notice, usually right away, is the strong similarity between the findings of positive psychology research and the guiding principles of twelve step recovery.
Positive emotions include a wide range of feelings, not just happiness and joy. Included are emotions like excitement, satisfaction, pride and awe, amongst others. These emotions are frequently seen as connected to positive outcomes, such as longer life and healthier social relationships.
Engagement refers to involvement in activities that draws and builds upon one’s interests. Mihaly Csikszentmihalyi explains true engagement as flow, a feeling of intensity that leads to a sense of ecstasy and clarity. The task being done needs to call upon higher skill and be a bit difficult and challenging yet still possible. Engagement involves passion for and concentration on the task at hand and is assessed subjectively as to whether the person engaged was completely absorbed, losing self-consciousness.
Relationships are all important in fueling positive emotions, whether they are work-related, familial, romantic, or platonic. We receive, share, and spread positivity to others through relationships. They are important in not only in bad times, but good times as well. In fact, relationships can be strengthened by reacting to one another positively. It is typical that most positive things take place in the presence of other people.
Meaning is also known as purpose, and prompts the question of “Why?” Discovering and figuring out a clear “why” puts everything into context from work to relationships to other parts of life. Finding meaning is learning that there is something greater than you. Despite potential challenges, working with meaning drives people to continue striving for a desirable goal. The three criteria are that it 1) contributes to well-being, 2) is pursued for its own sake, and 3) is measured independently of the other elements of PERMA.
Accomplishments are the pursuit of success and mastery. Unlike the other parts of PERMA, they are sometimes pursued even when it does not result in positive emotions, meaning, or relationships. Accomplishment can activate the other elements of PERMA, such as pride under positive emotion.Accomplishments can be individual or community based, fun or work based.
The five domains are valuable to consider when "the program isn't working," because taking personal inventory usually comes down to looking at what's going on inside these categories. The five elements were sifted out of research on thousands of individuals who were interviewed on the broad topic of happiness.
Change Your Brain
BRAINHEALTH PHYSICALS
A unique cognitive assessment that measures cognitive reserve in pivotal areas of higher-order mental functioning, all of which rely on robust frontal lobe function. It is just as essential to measure and monitor brain fitness as it is to measure and monitor physical fitness. Get a benchmark of your brain’s health.
HIGH PERFORMANCE BRAIN TRAINING
The high performance brain training program, Strategic Memory Advanced Reasoning Training (SMART®
I joined the staff at The Center for BrainHealth and BPI after extensive contact with the scientists and clinicians there. Over a period of months I found myself returning at least once or twice weekly to attend a lecture, to discuss research, or to interact with my friends on The Warrior Team, a powerful resource for veterans. I remember the day in November 2014 when I spoke with Dr. Sandra Chapman, the CEO, and she asked me whether I was enjoying my visits. "Are you kidding me?" I said, "I want to be more than a visitor—I want to work here!" Needless to say, I was both honored and extremely delighted when, early in 2015, I got the call and the invitation to be Senior Medical Advisor for CBH and BPI.
Beliefs Shape Our Reality
Surprisingly large numbers of people also hold beliefs that a psychiatrist would class as delusional. In 2011, psychologist Peter Halligan at Cardiff University assessed how common such beliefs were in the UK (see below for the top 10 delusions). He found that more than 90 per cent of people held at least one, to some extent. They included the belief that a celebrity is secretly in love with you, that you are not in control of some of your actions, and that people say or do things that contain special messages for you (Psychopathology, vol 44, p 106).
None of Halligan's subjects were troubled by their strange beliefs. Nonetheless, the fact that they are so common suggests that the "feeling of rightness" that accompanies belief is not always a reliable guide to reality.
The Top 10 Delusions
1. Your body, or part of your body, is misshapen or ugly 46.4%
2. You are not in control of some of your actions 44.3%
3. You are an exceptionally gifted person that others do not recognise 40.5%
4. Certain places are duplicated, i.e. are in two different locations at the same time 38.7%
5. People say or do things that contain special messages for you 38.5%
6. Certain people are out to harm or discredit you 33.8%
7. Your thoughts are not fully under your control 33.6%
8. There is another person who looks and acts like you 32.7%
9. Some people are duplicated, i.e. are in two places at the same time 26.2%
10. People you know disguise themselves as others to manipulate or influence you 24.9%
One of the most interesting things about belief is that it varies enormously from person to person, especially on issues that really matter such as politics and religion. According to research by Gerard Saucier of the University of Oregon, these myriad differences can be boiled down to five basic "dimensions" (Journal of Personality and Social Psychology, vol 104, p 921). At their core, he says, these concern what we consider to be worthy sources of value and goodness in life, whether it be a concept, an object, a supernatural being or a historical person. Your belief system is the aggregate of your position on each of these five dimensions, which are independent of each other.
1. Traditional religiousness: level of belief in mainstream theological systems such as Christianity and Islam
2. Subjective spirituality: level of belief in non-material phenomena such as spirits, astrology and the paranormal
3. Unmitigated self-interest: belief in the idea that hedonism is a source of value and goodness in life
4. Communal rationalism: belief in the importance of common institutions and the exercise of reason
5. Inequality aversion: level of tolerance of inequality in society, a proxy of the traditional left-right political split
To read the full article, click here.
Identifying the Effective Psychiatrist
Practicing medicine is a privilege granted to very few individuals, and I am indeed fortunate. Within the field of medicine, working in psychiatry requires more than an understanding of anatomy and organ systems, because psychiatry is about the mind, the brain, the self, and human experience.
Like any other professional, I believe in high ethical standards, sound knowledge of my field, and the importance of practicing wisely and compassionately. Beyond the obvious nostrums and philosophical cliches, however, I want to be one of the good psychiatrists. As I thought about this lately, I began to wonder: how does one identify and recognize a really good psychiatrist? What makes a good psychiatrist? If I made a list of the most important aspects of a psychiatrist’s professional philosophy, what would that look like?
In 2006 an article was published in the Journal of Affective Disorders showing that good psychiatrists prescribing placebos (sugar pills) had better results than poor psychiatrists prescribing actual medication. Over 120 patients were divided into two groups, one group that received sugar pills and another group that received full strength psychiatric medication for depression. At the same time, each psychiatrist was rated on a number personal qualities: verbal fluency, interpersonal perception, expressiveness, warmth, acceptance, empathy, and the ability to focus on the other person. When results were analyzed, the psychiatrists strong in these personal qualities had the best results, even when the “medication” they prescribed was not medication at all.
The effective psychiatrists were fluent, clear, and expressive in speaking, and they had an accurate feel for their patients. Rather than being distant and aloof, the good psychiatrists were warm, friendly, and accepting. The good psychiatrists empathized well, spent more time with their patients, were more thoughtful in their strategies, and formed strong therapeutic partnerships. The point of the study was that having a good psychiatrist makes a difference in recovery.
Although medication can be extremely helpful in psychiatric care, treatment is not all about medication. The combination of the right medication, the right psychotherapy, and the right psychiatrist is the key to success.
Research has shown for generations that some clinicians consistently produce better results than others, regardless of the type of psychotherapy or theoretical orientation of the practitioner. Hundreds of studies have shown that the differences between types of psychotherapy is very small, but the psychiatrist providing the psychotherapy is critically important.
Over the past fifteen years, extensive research has given us a solid body of evidence about the qualities and actions of effective psychiatrists. Based on the psychotherapy research of Dr. Bruce Wampold of The University of Wisconsin, I have formulated here an inventory that provides the basis for judging whether a psychiatrist is likely to be effective.
- Effective psychiatrists demonstrate a sophisticated set of interpersonal skills, including verbal fluency, perceptiveness of others, emotional intelligence, expressiveness, warmth, and acceptance. Given these gifts, the most effective psychiatrists are those who are first excellent physicians, well trained in medicine, competent to practice at the highest levels.
- Effective psychiatrists are inquisitive, questioning, and seeking new knowledge constantly. They embrace science while at the same time possessing the humility to know how little we really know.
- Patients of effective psychiatrists feel understood, trust the psychiatrist, and believe the psychiatrist can help. The psychiatrist creates these conditions in the first moments in both speech and action. In the initial contacts, patients are very sensitive to cues of acceptance, understanding, and expertise. Although these conditions are necessary throughout therapy, they are most critical in the initial interaction to ensure engagement in the therapeutic process.
- Effective psychiatrists are able to form a working alliance with a broad range of patients. The working alliance involves the therapeutic bond, but also importantly agreement about the task of goals of therapy. The working alliance is described as collaborative, purposeful work on the part of the patient and the psychiatrist. The effective psychiatrist builds on the patient’s initial trust and belief to form this alliance and the alliance becomes solidly established early in therapy.
- Effective psychiatrists provide an acceptable and practical explanation for the patient’s distress. The patient wants an explanation for his or her symptoms or problems. There are several considerations involved in providing the explanation. First, the explanation must be consistent with the healing practice. On the medical side, the explanation is biological, and in psychotherapy the explanation is psychological. Second, the explanation must be acceptable and compatible with the patient’s attitudes, values, culture, and worldview. Third, the explanation must provide a strategy by which the patient can overcome difficulties and solve life’s problems. These three factors together make for a strong therapeutic alliance.
- The effective psychiatrist provides a treatment plan that is consistent with the explanation provided to the patient. Once the patient accepts the explanation, the treatment plan will make sense and patient compliance will be increased. The treatment plan must involve healthy actions—the effective psychiatrist promotes healing by replacing failed strategies with effective strategies. At the same time, strong defenses will replace weak defenses, and healthy practices will replace self-defeating behaviors.
- The effective psychiatrist is influential, persuasive, and convincing. The psychiatrist presents the explanation and the treatment plan in a way that convinces the patient that the explanation is correct and that following through with the treatment will benefit the patient. This process leads to patient hopefulness, increased expectancy for mastery, and healthy actions. These characteristics are essential for forming a strong working alliance.
- The effective psychiatrist is honest and authentic. Authenticity refers to communication to the patient that the psychiatrist truly wants to know how the patient is doing. The best psychiatrists tend not to use checklists, scales, and paper measures. Instead, they talk and listen openly and honestly.
- The effective psychiatrist is flexible and will be patient if resistance to the treatment is apparent or the patient is slow to make progress. Although the effective psychiatrist is persuasive, persuasion can be a process that takes time. The good psychiatrist pays attention, takes in new information, test hypotheses about the patient, and is willing to be wrong. A good psychiatrist will seek second opinions, refer to other specialists, and even take calculated risks such as trying a new approach or a newly released medication.
- The effective psychiatrist does not avoid difficult material in therapy. Doctor and patient must use such difficulties therapeutically. We all tend to avoid material that is difficult. The effective psychiatrist senses avoidance is taking place and does not collude to avoid the material. Instead, the psychiatrist will discuss the difficult material and address difficult problems. Sometimes conversations can be difficult, and at times the relationship between doctor and patient can be strained, but this is part of the work of therapy. The good psychiatrist can use skill, experience, and compassion to overcome these barriers to recovery.
- The effective psychiatrist communicates hope and optimism. Sometimes this is easy to do, and sometimes it’s difficult. The working partnership must maintain hope and optimism in the face of chronic illness, relapses, lack of consistent progress, and many other difficulties. Effective psychiatrists acknowledge these issues and still communicate hope that the patient will achieve realistic goals in the long run. This communication is not blind faith or Pollyanna optimism, but rather a firm belief that together the psychiatrist and patient will work successfully. At the same time, effective psychiatrists mobilize patient strengths and resources to facilitate the patient’s ability to solve his or her own problems. The best doctors know that the patient, through his or her work, is responsible for therapeutic progress, creating a sense of mastery.
- Effective psychiatrists are aware of the patient’s characteristics and context. This is a tall order with many categories: culture, race, ethnicity, spirituality, sexual orientation, age, physical health, motivation for change, and beyond. Furthermore, the effective psychiatrist is aware of how his own background, personality, and beliefs figure into the relationship.
- The effective psychiatrist is aware of his or her own psychological process and does not inject his or her own material into the therapy process unless such actions are deliberate and therapeutic.
- The effective psychiatrist is aware of the best research evidence related to the particular patient, in terms of treatment, problems, and social context. It is very important to understand the biological, social, and psychological basis of the patient’s problem.
- The effective psychiatrist seeks always to improve, always to be a student. Hippocrates said, “The life so short, the craft so long to learn,” and truer words were never spoken.
- Finally, the good psychiatrist must possess both humility and a sense of humor. We will never know enough, or be wise enough, to have all the answers. We cannot take ourselves too seriously, lest we become arrogant, prideful, and set ourselves apart from those who have graced us with the privilege of being socially sanctioned healers.
Development of skill in psychiatry involves intensive practice and unceasing professional growth. Patients are sometimes our best and most effective teachers. A few years ago I taught a seminar for third year students at the University of Texas Southwestern Medical School, “Psychiatric Nightmares, Disasters, and Catastrophes.” The entire content of the seminar consisted of mistakes I’d made, errors I had committed, and pitfalls that these students likely would encounter, sooner or later, in their medical careers.
I told the story of a patient with whom I’d had a terrible, angry argument, and how guilty I felt for years about my lack of composure—only to have the patient return, two years later, to ask me for a job at the hospital and tell me that she had been shaken into reality by our confrontation. I told them the story of the patient who overdosed and came to the ICU, and how I was baffled by the case—until I realized that the patient had diabetes, and was actually in a diabetic coma, not a drug-induced state.
I told them about the patient who came to the doorstep of my home on a Sunday afternoon, bearing in her arms her injured pet cat, hoping that I could help. I told them about an elderly man from New Orleans who was my patient in the middle of the night as Hurricane Katrina washed away his home.
And I told them about the time when I was called to the ER to examine a beautiful young woman, a Duke University cheerleader, who had bruised her shoulder. When I approached her to examine the injury, and she undid her gown and dropped it with a smile, I calmly reached into the pocket of my white coat for my stethoscope, only to realize that I then stuck my reflex hammer in my ear.
These encounters are the building blocks of the effective psychiatrist’s life. I’ve come to realize that most of the learning happens after we graduate. As Dr. Stead used to say at Duke, “Medical school is where you stay for four years until you’re old enough to become a doctor.”
Treatment Philosophy
My approach to psychiatric practice reflects many years studying human nature and working to help people who are having a hard time in life. By the time most people see a psychiatrist, they are worried, or they are sad, or they are very confused about something I will just call “the problem,” or “the complaint.” Let me make some general comments about my approach, and then I will discuss my thinking on the use of medications.

People seek psychiatric help for a variety of problems, but everyone wants the same result: to feel better, to think more clearly, to rediscover satisfaction and happiness, and to regain a sense of self control and personal freedom. The problem may be related to mood, energy level, motivation, sleep, worry, relationships, anger, troubled behavior, obsessions, compulsions -- it’s a long list. People who drink too much, use drugs, or misuse prescription medication are often using these chemicals to find relief. Alcoholism and substance abuse are widespread in our culture.
Dealing with life is never easy.
Most persons first try to solve the problem or deal with the complaint on their own. Frustrated that things aren’t improving, they may seek advice from others. Sometimes a person hides the problem or lives in silence with the complaint. They may read a book, go to a support group, consult the internet, or try a new religious practice. We all have problems and complaints, and we all do the best we can to solve the dilemmas of life. When someone calls me about consultation, I almost always hear them say that they have a problem, they have tried to solve the problem, and they are looking for someone who knows how to help make things better.
One of the individuals consulting with me said, “I feel like I’m in a box, and the directions for getting out of the box are printed -- on the outside of the box.”
A successful airline pilot, a Vietnam combat veteran, said, “Doc, I’m out of altitude, airspeed, and ideas.”
Often the person seeking help has waited so long that demoralization has begun to set in, and they are beginning to lose hope. This doesn’t mean that the individual is suicidal or, in fact, any more unhappy than many of the people at the workplace or in the neighborhood. It means that they are resigned to always feeling this way, never feeling any better than this. Demoralization means a state of mind in which a person considers accepting fate, giving up, and abandoning the idea that things can get better.
Fear, anger, resentment, feeling constantly wounded, feeling overwhelmed, feeling unappreciated, feeling worthless -- all of these emotions are part of our lives. But when we feel negative all the time, or most of the time, most days, then we need help. There are very few emotional problems that defy intelligent therapy and reasonable efforts toward a solution.
When I meet someone for the first time in consultation, I have three major concerns. First, I want to get to know the person and hear about the problem are the complaint. My first question usually is simply, “How can I help?” or “What brings you to see me?” Second, I want to explore the individual’s point of view or understanding of the problem, including what solutions have been attempted. Third, I want to consider what we can do, working together, to improve the situation. I tend to focus more on results than on reasons. I’m not always sure about why things happen, but I am very focused on what we can do now. Sometimes I explain in detail how the brain works, and sometimes I discuss how life works. The process of recovery involves growth, change, and even personal transformation.
Research shows that psychotherapy can help, medication can help, and intelligent problem solving helps. Psychotherapy is not for everyone, and medication is not for everyone, but the vast majority of people who want help can find it. One of my favorite expressions is, “You have to do it yourself, but you can’t do it alone.”
Over the years I have developed a style that I call “sober conversation.” The word “sober” does not apply just to alcohol and addictions. To be sober is to be serious, to focus on what is most important, and to try to get it right. I believe in the importance of what we care about, and in this regard I have seriously studied the specific problem of human will. I call it “the problem of human will” because we are often confused about what we will ourselves to do, or not to do. When I work as a psychotherapist, I am most interested in what people care about, how their beliefs and assumptions about life have been formed, and where they feel stuck or at odds with themselves. Sometimes we have conflicting feelings about the same thing. For example, someone wants to take life in a certain direction, but he or she feels conflicted about it. Or someone tries to solve a problem, not realizing that it’s part of a bigger problem, or a different kind of problem. My definition of psychotherapy is that it is a form of personal consultation, focused on the situation of the client, with the goal of solving problems and feeling better.

Not everyone is cut out for in-depth or long-term conversation. Some people like to come for a few visits, and some like to keep going for weeks, or even months on a weekly basis. Some people prefer to come two or three times a week because they want to do the work and get on with whatever is next. Some people come for an hour, and some come for an afternoon.
Psychotherapy does take time, because the process is basically two people getting to know each other in the context of a specific purpose. Psychotherapy at its best is about taking life seriously, getting it right, and feeling the satisfaction that comes from clarity of thought, commitment to integrity, and comfort with the complexity of one’s own emotions and ideas. Some say that psychotherapy is a dying art, and this may be true. Psychiatrists today (and perhaps psychologists as well) do not receive the extensive training in psychotherapy that we did thirty years ago. Many psychiatrists and psychologists are not interested in psychotherapy. And many psychotherapists are not really very good or very well trained. Today there are thousands of people who call themselves “life coaches,” and anyone can hang out a shingle and call himself a “life coach.” There are several private organizations that offer “certifications,” but there are no license requirements, there is no government regulation, and no educational standard that is generally accepted. For these reasons, I think the concept makes sense, but in practice let the buyer beware -- caveat emptor!
Medications can be very helpful in treating some specific psychiatric problems. Today we have excellent medications for anxiety, depression, moodswings, insomnia, attention deficit disorder, and other conditions. Bipolar disorder, for example, is a devastating condition that can be very effectively managed with medication, restoring individuals to a life of normalcy and stability. I have absolutely no doubt about the value of psychiatric medications. I also believe that what is most important is getting the right diagnosis and the correct strategy for intervention and treatment. I see many people who have been misdiagnosed, and even mistreated, because they have not been well assessed. Assessment can take time, and I never jump to conclusions about diagnosis. After knowing someone for a few weeks, together we may decide that we see the condition in a different way.
Psychiatric medications are powerful, effective tools when used properly, but they also have side-effects, and they are expensive. Getting the right medication for the right diagnosis is extremely important. And there is an old saying from Hippocrates, creator of The Hippocratic Oath: “It is more important to know what sort of person has a disease than to know what sort of disease a person has.“