Painkillers: New Guidlines
Opioid painkillers such as OxyContin and Vicodin are now prescribed to as much as 4% of the U.S. population — 250 million prescriptions — with their use quadrupling since 1999. Some 1.9 million Americans are now addicted to, or dependent on, the painkillers. And from 1999 to 2014, about 165,000 people died of overdoses. Almost all of the opiate-related drugs on the market for pain are as addictive as heroin.
According to the National Institute on Drug Abuse (NIDA), the abuse of and addiction to opioids such as heroin, morphine, and prescription pain relievers is a serious global problem that affects the health, social, and economic welfare of all societies. It is estimated that between 26.4 million and 36 million people abuse opioids worldwide, with an estimated 2.1 million people in the United States suffering from substance use disorders related to prescription opioid pain relievers in 2012 and an estimated 467,000 addicted to heroin. The consequences of this abuse have been devastating and are on the rise. For example, the number of unintentional overdose deaths from prescription pain relievers has soared in the United States, more than quadrupling since 1999. There is also growing evidence to suggest a relationship between increased non-medical use of opioid analgesics and heroin abuse in the United States.
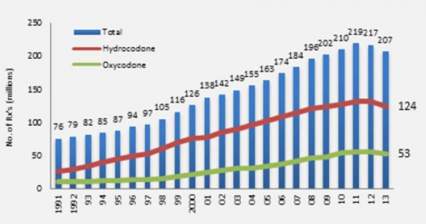
Increase in Opioid Prescriptions 1991-2013
Opioid medications can produce a sense of well-being and pleasure because these drugs affect brain regions involved in reward. People who abuse opioids may seek to intensify their experience by taking the drug in ways other than those prescribed. For example, extended-release oxycodone is designed to release slowly and steadily into the bloodstream after being taken orally in a pill; this minimizes the euphoric effects. People who abuse pills may crush them to snort or inject which not only increases the euphoria but also increases the risk for serious medical complications, such as respiratory arrest, coma, and addiction. When people tamper with long-acting or extended-release medicines, which typically contain higher doses because they are intended for release over long periods, the results can be particularly dangerous, as all of the medicine can be released at one time. Tampering with extended release and using by nasal, smoked, or intravenous routes produces risk both from the higher dose and from the quicker onset.
The Centers for Disease Control released a dozen opioid prescription guidelines in the Journal of the American Medical Association (JAMA). They will not have the power of law but will guide insurance company recommendations to doctors and Veterans Administration prescriptions for retired military patients, with the aim of curbing dangerous prescribing practices. "Primary care clinicians find managing chronic pain challenging," according to JAMA, and "evidence of long-term efficacy of opioids for chronic pain is limited. Opioid use is associated with serious risks, including opioid use disorder and overdose."
The guidelines are based on three principles. First, opioids should be a last option for these patients, with aspirin-related drugs and exercise preferred. Second, when given, doses should start out low and only increase slowly. Third, patients should be monitored and a plan for getting them off the drugs should start with their prescription. The guidelines also call for getting naloxone, a drug used to counteract overdoses, into the hands of more doctors, nurses, police, and emergency personnel.
CASA Report on Addictions
CASA Columbia’s work for this report involved:
• A review of more than 7,000 publications
• Analyses of 5 national data sets
• Interviews with and suggestions from 176 leading experts in a broad range of fields relevant to the report
• Focus groups and a national general population survey of 1,303 adults about their attitudes and beliefs related to addiction and its treatment
• Two New York State surveys of addiction treatment providers
• An online survey of 1,142 members of professional associations involved in addiction care
• An online survey of 360 individuals with a history of addiction
• Analyses of state and federal governments’ and professional associations’ licensing and certification requirements for treatment providers
• A case study of addiction treatment in New York State and New York City
This 5-year study found that, despite the prevalence of addiction, the enormity of its consequences, the availability of effective solutions and the evidence that addiction is a disease, both screening and early intervention for risky substance use are rare, and only about 1 in 10 people with addiction involving alcohol or drugs other than nicotine receive any form of treatment.
Of those who do receive treatment, few receive anything that approximates evidence-based care. This compares with 70% to 80% of people with such diseases as high blood pressure and diabetes who do receive treatment. This report exposes the fact that most medical professionals who should be providing addiction treatment are not sufficiently trained to diagnose or treat the disease, and most of those providing addiction care are not medical professionals and are not equipped with the knowledge, skills or credentials necessary to provide the full range of effective treatments. Misunderstandings about the nature of addiction and the best ways to address it, as well as the disconnection of addiction medicine from mainstream medical practice, have undermined effective addiction treatment.
CASA Recommendations: The time has come for addiction medicine to be fully integrated into health care systems and medical practice. Health care providers, especially physicians, are our front line in disease prevention and treatment. They must understand the risk factors for addiction, screen for risky substance use and intervene when needed, and diagnose, treat and manage addiction just as they do all other diseases.
Other health care providers, including nurse practitioners, physician assistants, psychologists and social workers, are critical parts of the solution as well. We need national, evidence-based standards that stipulate who may provide addiction treatment, and core competencies for all health care providers integrated into their education and licensing requirements. We must regulate addiction treatment facilities and programs as health care providers and hold them accountable for treatment consistent with medical standards and proven practices.
Adderall Time in Texas
Here at the office, where I answer my own phone (and do my best to return all calls myself) I receive 4-5 calls weekly from individuals looking for a doctor who will prescribe Adderall or its long-acting cousin, Vyvanse (Lisdexamfetamine). Curious as it seems, many callers say that they are new to Dallas and need a new doctor to prescribe the medication. I say this is curious for two reasons. First, let's say that a doctor outside of Texas has a patient who is moving to Texas. One thing that prescribing doctor should do is help his or her patient to refer the individual to a reliable doctor in the new city; and apparently, many doctors from other states don't do this. Second, people taking stimulants don't usually have serious withdrawal problems, but coming off stimulants like Adderall can pose problems, because the person's brain has to adjust rapidly to the absence of the drug. The person who depends on Adderall will probably feel lethargic and "flat" when they don't have the medication on board. Students often panic, fearing they won't be able to study or put in the long hours required for academic performance.
As with other potentially risky medications (like Xanax, hydrocodone, oxycodone, etc.), the prescribing physician assumes certain risks and responsibilities in writing the prescription. I worry about this. Many patients tell me that they have only seen the doctor 3-4 times a year, and some say that they don't even see a doctor, because a mid-level practitioner (usually a nurse practitioner) writes the prescriptions under the "supervision" of a medical doctor. The typical "med check" or brief visit to renew a prescription lasts less than 20 minutes. This is not necessarily bad or wrong, but we certainly have to wonder whether the responsible doctor really knows very much about the patient. The Texas Medical Association has noted that authorities are cracking down on "pill mill" physicians in pain management clinics, and it's very likely that doctors prescribing other Schedule II ("dangerous") drugs will face similar scrutiny.
My expert opinion is that medications are very helpful in the treatment of attention deficit disorder. My further opinion is that many people, particularly students and younger adults, are using these medications inappropriately. This is one reason that I answer my own phone. I hate it when someone shows up expecting me to write controlled substances without any discussion. Yes, these are good medications that really help many people. And no, I won't write a Schedule II medication unless there's compelling clinical evidence that justifies the prescription.
Update 10/17/15: I have been reading commentaries by Larry Diller, M.D., a developmental pediatrician who has written extensively about stimulants. He has strong and generally well-informed opinions about the use and misuse of medications like Adderall, Vyvanse, Ritalin, and Concerta. His website and his opinions can be found here.
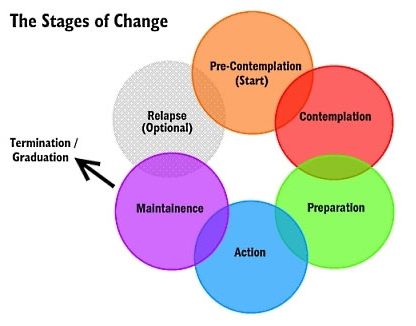
Stages of Change: A Summary
Stages of Change
The Stages of Change, as described in the treatment of alcoholism and other addictions, can be summarized in five parts. The stages are best conceptualized as a cycle. Alcoholics and addicts cycle through the stages, sometimes three or four times, before they complete the cycle without a slip or a relapse. This can be very frustrating for all concerned. But that's the nature of the game.
1) PRECONTEMPLATION STAGE
"It isn't that we can't see the solution. It's that we can't even see the problem for what it is."
Pre-contemplators usually show up in therapy because of pressures from others: spouses, employers, parents, and courts. They resist change. When their problem comes up, they change the topic of conversation. They place responsibility for their problems on factors such as genetic makeup, addition, family, society, destiny, the police. They explain how little they actually use or drink, and they complain that no one gives them credit when they cut down or even abstain for a short time. They feel hopeless and demoralized, and they are often defensive, angry, and frankly illogical in their thinking.
2) CONTEMPLATION STAGE
"I want to stop feeling so stuck. I am tired of all the hassles and of other people intruding in my life."
Contemplators admit that they have a problem and begin to think about solutions. Contemplators struggle to understand their problems, to see its causes, and wonder about possible solutions. Many contemplators have indefinite plans to take action within the next few months. They know where they want to do, and they have ideas (some good, some not so good) about how to get there.
"You know your destination, and maybe even how to get there, but you're not ready to go…yet."
Contemplators tell themselves that someday they are going to change. When contemplators are trying to reach the preparation stage of change, their thinking is clearly marked by two changes.
First, they begin to think more about the future than the past.
The end of contemplation stage is a time of anticipation and anxiety. Relapse is common when individuals reach this stage. They are fearful of what will happen next. Support from family and friends may be exhausted. Even though they have made considerable effort, things often don't get easier — not yet.
Between stage 2 and 3: A decision is made. People conclude that the negatives of their behavior outweigh the positives. They choose to change their behavior. They make a commitment to change. This decision represents an event, not a process.
3) PREPARATION STAGE
Most people in the preparation stage are planning to take action and are making the final adjustments before they begin to change their behavior. Usually they have not resolved their ambivalence. A part of them wants to get well, but as the Zen saying puts it, "The mind is a barrel of wild monkeys," and they often go back and forth about taking action.
4) ACTION STAGE
The time for action does not come on with a blinding flash of light. There is no burning bush. Gradually the person overtly modifies his or her behavior and his or her surroundings. At this point the make the move for which they have been preparing. This is a critical point, and it requires the greatest commitment of time and energy.
Change is visible to others. Others can see the difference in attitude, honesty and commitment. Small changes sometimes matter the most.
5) MAINTENANCE STAGE
Change never ends with a single action. One old saying in Alcoholics Anonymous is that without a strong commitment to maintenance, there will surely be relapse, usually to the pre-contemplation or contemplation stage.
THE IMPORTANCE OF PROCESSES
Processes are selected activities that are regularly initiated to effect change. There are nine important ones chosen by therapists as distinct areas of consideration and useful tools in personal transformation.
1. Consciousness-raising: Increasing knowledge about yourself and your problem.
2. Social liberation: Considerations in the external environment that can contribute to helping change, i.e.: no smoking areas, lo-cal menu items, advocacy groups.
3. Emotional arousal: Increased awareness through depth of feeling from natural events or dramatic intervention, psychodrama.
4, Self-reevaluation: A thoughtful and emotional reappraisal of yourself as regards your problem, weighing the pros and cons of changing.
5. Commitment: Acknowledging that you are the only one who can respond, speak and act for yourself.
6. Countering: Planning for and substituting healthy responses for unhealthy ones, action oriented.
7. Environmental control: Restructuring your personal environment so that the probability of a problem-causing event is reduced.
8. Rewards: Affirmation of desirable behavior by self or others as contrasted with and better than any type of punishment for problem behavior.
9. Helping relationships: Receiving care, support and assistance from significant people in your life.
For more information about the stages of change, see the book Changing for Good by James Prochaska.
Painkiller Overdoses On the Rise
This news isn’t shocking to those of us who encounter addiction daily, but it’s in the headline today at USA Today. Other items of note from today’s paper:
With nearly 44,000 deaths a year, more Americans today die from drug overdoses than from car accidents or any other type of injury. Many of these deaths could be prevented if patients had better access to substance abuse therapy, experts say. Yet people battling addiction say that treatment often is unavailable or unaffordable.
Only 11% of the 22.7 million Americans who needed drug or alcohol treatment in 2013 actually got it, according to the Substance Abuse and Mental Health Services Administration. While some of those who went without care did so by choice, at least 316,000 tried and failed to get treatment.
"We know addiction treatment saves lives, reduces drug use, reduces criminal activity and improves employment," says Paul Samuels, president and director of the Legal Action Center, which advocates on behalf of people with HIV or addiction. "The data is there, the evidence is in, but our public policy has not caught up with the science."
Meanwhile, the crisis is getting worse, says Thomas Frieden, director of the Centers for Disease Control and Prevention. The death rate from drug overdoses more than doubled from 1999 to 2013, according to the CDC. The bulk of these deaths involve opiates, a class of pain killers that includes morphine and Oxycontin.
Injection drug use has fueled an outbreak of HIV in rural Indiana, a nationwide surge in hepatitis C infections, and an increase in the number of babies born addicted to drugs. States have responded to the surge in overdose deaths by expanding access to naloxone, a fast-acting rescue drug that can reverse the effects of an opiate overdose. Indiana lawmakers also voted to allow needle exchange programs in communities facing a public health crisis related to injection drug use. While those approaches are welcome, they don't treat the underlying addiction.
The wait for a spot in a detoxification program ranges from days to weeks, and it can be very expensive. As I say elsewhere here on my site, it's also true that not all treatment is really good treatment. Consumers are disadvantaged twice. Not only is treatment hard to find in the first place, but it's hard to know what constitutes a good treatment program. I have some comments about this on my FAQ page and on my Philosophy page.