Being Mindful: Getting Started
Find a good spot in your home or apartment, ideally where there isn’t too much clutter and you can find some quiet. Leave the lights on or sit in natural light. You can even sit outside if you like, but choose a place with little distraction.
At the outset, it helps to set an amount of time you’re going to “practice” for. Otherwise, you may obsess about deciding when to stop. If you’re just beginning, it can help to choose a short time, such as five or ten minutes. Eventually you can build up to twice as long, then maybe up to 45 minutes or an hour. Use a kitchen timer or the timer on your phone. Many people do a session in the morning and in the evening, or one or the other. If you feel your life is busy and you have little time, doing some is better than doing none. When you get a little space and time, you can do a bit more.
Take good posture (see instructions above with actor Sandra Oh above) in a chair or on some kind of cushion on the floor. It could be a blanket and a pillow, although there are many good cushions available that will last you a lifetime of practice. You may sit in a chair with your feet on the floor, loosely cross-legged, in lotus posture, kneeling—all are fine. Just make sure you are stable and erect. If the constraints of your body prevent you from sitting erect, find a position you can stay in for a while.
When your posture is established, feel your breath—or some say “follow” it—as it goes out and as it goes in. (Some versions of the practice put more emphasis on the outbreath, and for the inbreath you simply leave a spacious pause.) Inevitably, your attention will leave the breath and wander to other places. When you get around to noticing this—in a few seconds, a minute, five minutes—return your attention to the breath. Don’t bother judging yourself or obsessing over the content of the thoughts. Come back. You go away, you come back. That’s the practice. It’s often been said that it’s very simple, but it’s not necessarily easy. The work is to just keep doing it. Results will accrue.
The Brain: A Good Introduction
The brain is the most complex organ in the human body. It produces our every thought, action, memory, feeling and experience of the world. This jelly-like mass of tissue, weighing in at around 1.4 kilograms, contains a staggering one hundred billion nerve cells, or neurons.
The complexity of the connectivity between these cells is mind-boggling. Each neuron can make contact with thousands or even tens of thousands of others, via tiny structures called synapses. Our brains form a million new connections for every second of our lives. The pattern and strength of the connections is constantly changing and no two brains are alike.
It is in these changing connections that memories are stored, habits learned and personalities shaped, by reinforcing certain patterns of brain activity, and losing others. To read the article, click here.
New Videos Added Today
4/26/2015
New in the media section: videos by Dr. Sandi Chapman, Dr. Ian Robertson, Dr. Howard Somers. Topics include a TED talk, an interview with the parents of a distinguished veteran who committed suicide, and a talk on "The Winner Effect."
Those Danged Cognitive Distortions
1. ALL-OR-NOTHING THINKING: You see things in black-and-white categories. If performance falls short of perfect, you see yourself or others as total failures.
2. OVERGENERALIZATION: You see a single negative event as a never-ending pattern of defeat. Phrases like "You always …" or "You never …" exemplify overgeneralization.
3. MENTAL FILTER: You pick out a single negative detail and obsess on it so that your vision of all reality becomes darkened, like the drop of ink that discolors an entire glass of water.
4. DISQUALIFYING THE POSITIVE: You reject positive experiences by insisting they "don't count" for some reason or other. In this way you can maintain a negative belief that is contradicted by your everyday experiences. Often this manifests as making excuses when somebody pays you a compliment.
5. JUMPING TO CONCLUSIONS: You make a negative interpretation even though there are no definite facts that convincingly support your conclusion often a "wait and see" attitude is called for in these situations.
• MIND READING: You arbitrarily conclude (usually by personalizing their behavior) that someone is reacting negatively to you, and you don't bother to check this out.
• THE FORTUNE TELLER ERROR: You often anticipate that things will turn out badly, and you feel convinced that your prediction is an already-established fact.
6. MAGNIFICATION (CATASTROPHIZING) OR MINIMIZATION: You exaggerate the importance of things (such as your achievements or someone else's goof up), or you inappropriately shrink things until they appear tiny (your own character defects or other people's acceptable behavior). This is also called the "binocular trick."
7. EMOTIONAL REASONING: You allow your negative emotions to color how you see the world with an "I feel it, therefore it must be true."
8. SHOULD STATEMENTS: You try to motivate yourself or others with should and shouldn't, as if needing be whipped and punished before you could be expected anything. "Musts" and "oughts" are also offenders. The emotional consequences are guilt. When you
direct should statements toward others, you feel anger, frustration, and resentment as do they!
9. LABELING AND MISLABELING: This is an extreme form of overgeneralization. Instead of describing your error, you attach a negative label to yourself. "I'm a loser." When someone else's behavior rubs you the wrong way, you attach a negative label to him "He's a dumb jerk!" Mislabeling involves describing an event with language that is highly colored and
emotionally loaded, and generally not factually descriptive.
10. PERSONALIZATION: You see yourself as the cause of some negative external event, which in fact you were not primarily responsible for.
My generation of psychiatrists was the first to break with the old-fashioned, unscientific model known as Freudian psychoanalysis—the stereotype of the patient lying on the couch for years and being "analyzed" by the shrink. For some reason, our generation just didn't see this as very helpful or useful. Psychoanalysis in its pure form means 4-5 visits a week to the psychoanalyst, and the typical course of therapy is measured in years! There were no outcome studies proving the effectiveness of this approach. We really wanted something that would produce results, and an approach that the average person could afford.
Dr. Ben Martin at PsychCentral describes the new, scientific talk therapy this way: Cognitive behavioral therapy (also known by its abbreviation, CBT) is a short-term, goal-oriented psychotherapy treatment that takes a hands-on, practical approach to problem-solving. Its goal is to change patterns of thinking or behavior that are behind people’s difficulties, and so change the way they feel. It is used to help treat a wide range of issues in a person’s life, from sleeping difficulties or relationship problems, to drug and alcohol abuse or anxiety and depression. CBT works by changing people’s attitudes and their behavior by focusing on the thoughts, images, beliefs and attitudes that we hold (our cognitive processes) and how this relates to the way we behave, as a way of dealing with emotional problems.
An important advantage of cognitive behavioral therapy is that it tends to be short, taking four to seven months for most emotional problems. Clients attend one session per week, each session lasting approximately 50 minutes. During this time, the client and therapist are working together to understand what the problems are and to develop a new strategy for tackling them. CBT introduces them to a set of principles that they can apply whenever they need to, and which will stand them in good stead throughout their lives.
Cognitive behavioral therapy can be thought of as a combination of psychotherapy and behavioral therapy. Psychotherapy emphasizes the importance of the personal meaning we place on things and how thinking patterns begin in childhood. Behavioral therapy pays close attention to the relationship between our problems, our behavior and our thoughts.
Yoga for PTSD in the Military
Notes on Club Drugs
How Are Club Drugs Abused?
GHB and Rohypnol are available in odorless, colorless, and tasteless forms that are frequently combined with alcohol and other beverages. Both drugs have been used to commit sexual assaults (also known as “date rape,” “drug rape,” “acquaintance rape,” or “drug assisted” assault) due to their ability to sedate and incapacitate unsuspecting victims, preventing them from resisting sexual assault.
GHB is usually ingested orally, either in liquid or powder form, while Rohypnol is typically taken orally in pill form. Recent reports, however, have shown that Rohypnol is being ground up and snorted. Both GHB and Rohypnol are also abused for their intoxicating effects, similar to other CNS depressants. GHB also has anabolic effects (it stimulates protein synthesis) and has been used by bodybuilders to aid in fat reduction and muscle building. Ketamine is usually snorted or injected intramuscularly.
How Do Club Drugs Affect the Brain?
GHB acts on at least two sites in the brain: the GABA receptor and a specific GHB binding site. At high doses, GHB’s sedative effects may result in sleep, coma, or death. Rohypnol, like other benzodiazepines, acts at the GABA receptor. It can produce anterograde amnesia, in which individuals may not remember events they experienced while under the influence of the drug.
Ketamine is a dissociative anesthetic, so called because it distorts perceptions of sight and sound and produces feelings of detachment from the environment and self. Ketamine acts on a type of glutamate receptor (NMDA receptor) to produce its effects, which are similar to those of the drug PCP. Low dose intoxication results in impaired attention, learning ability, and memory. At higher doses, ketamine can cause dreamlike states and hallucinations; and at higher doses still, ketamine can cause delirium and amnesia.
Addictive Potential
Repeated use of GHB may lead to withdrawal effects, including insomnia, anxiety, tremors, and sweating. Severe withdrawal reactions have been reported among patients presenting from an overdose of GHB or related compounds, especially if other drugs or alcohol are involved.
Like other benzodiazepines, chronic use of Rohypnol can produce tolerance, physical dependence, and addiction.There have been reports of people binging on ketamine, a behavior that is similar to that seen in some cocaine or amphetamine dependent individuals. Ketamine users can develop signs of tolerance and cravings for the drug.
What Other Adverse Effects Do Club Drugs Have on Health?
Uncertainties about the sources, chemicals, and possible contaminants used to manufacture many club drugs make it extremely difficult to determine toxicity and associated medical consequences. Nonetheless, we do know that: Coma and seizures can occur following use of GHB. Combined use with other drugs such as alcohol can result in nausea and breathing difficulties. GHB and two of its precursors, gamma butyrolactone (GBL) and 1,4 butanediol (BD), have been involved in poisonings, overdoses, date rapes, and deaths. Rohypnol may be lethal when mixed with alcohol and/or other CNS depressants. Ketamine, in high doses, can cause impaired motor function, high blood pressure, and potentially fatal respiratory problems.
What Treatment Options Exist?
Not many. These drugs are exotic and relatively rare compared to alcohol, meth, cocaine, marijuana, commonly abused prescription medications. As far as I know, there are no treatment programs specifically devoted to club or designer drugs. This can be a problem for the addict or drug abuse seeking help for these drugs. They enter residential or outpatient programs where other patients, and often most of the staff, don't know or understand the problems unique to this group of chemicals. My recommendation is for careful initial assessment—I discuss this at length in both the FAQ section and my philosophy of treatment section—so that an intelligent and individualized treatment approach is possible, and so the right intensive treatment program is selected when needed.
SMART Training for Teens
Teen SMART Camp is a great chance for your children or grandchildren to boost their frontal lobe functioning and gain important strategies for learning.
For questions and registration, please contact Lindsay Gehan at Lindsay.Gehan@utdallas.edu or 972.883.3310
Over the last six years, BrainHealth researchers have trained more than 27,000 students in SMART through research grants. Results have shown significant changes in frontal lobe regions responsible for higher order thinking and problem solving after only 10 hours of training. SMART has shown substantial improvements in academic performance in those who have participated to date.
SMART is a series of seven cognitive strategies that can be applied to any learning context. As students’ progress through these steps, they learn to discard unsuccessful and superficial learning styles and to adopt a more robust, focused, and deeper-level strategic learning approach. Upon completion of the SMART training, students can apply the methodology to any subject and have been shown scientifically to do so over an extended period of time with success.
This summer’s teens will begin SMART Camp by receiving comprehensive strategy instruction, teaching them to use their brains more efficiently to improve learning. SMART campers employ their new strategies in a variety of fun learning activities involving academic content as well as personally-relevant materials such as their favorite song lyrics, television shows, magazine articles, or movies, emphasizing organizational and motivational skills. The training is designed to help the teens apply their newly learned strategies to everyday situations. Each camper works on an individual and a group project over the course of the camp to practice planning, goal setting and time management.
The brain is primed for higher order reasoning beginning in adolescence. As a result, this SMART program is offered for students who will enter the 7th through 12th grade in Fall 2015.
SMART Camp has a maximum enrollment of 20 students and are filled on a first-come, first serve basis. The full payment amount is due before the camp begins.
Schedule:
June 22-26th 2015 – The day will start promptly at 9:00 am and conclude at 3:00 pm.
SMART Camp takes place over one week at the Center for BrainHealth.
Please contact Lindsay Gehan at Lindsay.Gehan@utdallas.edu or 972-883-3310 for more information
Science on Will and Willpower - Part II
An excellent video of one of Roy's lectures is on my media page.
We try to control ourselves in all sorts of ways: eating right, exercising, avoiding drugs and alcohol, studying more, working harder, spending less. Baumeister says that the practical significance of all this is enormous. He says: "Most of the problems that plague modern individuals in our society — addiction, overeating, crime, domestic violence, sexually transmitted diseases, prejudice, debt, unwanted pregnancy, educational failure, underperformance at school and work, lack of savings, failure to exercise — have some degree of self control failure as a central aspect."
Baumeister goes on to say that two main traits that seem to produce an immensely broad range of benefits: intelligence and self-control. However, psychology has not found much one can do to produce lasting increases in intelligence. On the other hand, self-control can be strengthened, and the study of self-control is a rare and powerful opportunity for psychology to make a palpable and highly beneficial difference in the lives of ordinary people.
For example, in his research he has found that people perform relatively poorly on tests of self-control when they have engaged in a previous, seemingly unrelated act of self-control: "For instance, in a study in my lab, we invited some students to eat fresh-baked chocolate-chip cookies, and asked others to resist the cookies and munch on radishes instead. Then we gave them impossible geometry puzzles to solve. The students who ate the cookies worked on the puzzles for 20 minutes, on average. But the students who had resisted the tempting cookies gave up after an average of eight minutes."
"Such studies suggest," he continues, "that some willpower was used up by the first task, leaving less for the second. The pattern is opposite to what one would expect based on priming or activating a response mode. So we began to think that some kind of limited resource is at work: It gets depleted as people perform various acts of self-control. Over time, we have begun to link this resource to the folk notion of willpower."
Making decisions seems to use up our willpower. After making decisions, people perform worse at self-control. Conversely, after exerting self-control, decision-making shifts toward simpler and easier processes. That can lead people to make poorer decisions, or to avoid making choices at all. Apparently, decision making depletes the same resource as self-control.
One of Baumeister's examples of willpower depletion: "A dieter may easily avoid a doughnut for breakfast, but after a long day of making difficult decisions at work, he has a much harder time resisting that piece of cake for dessert. Another example might be losing your temper. Normally, you refrain from responding negatively to unpleasant things your romantic partner says. But if one day you’re especially depleted — maybe you’re trying to meet a stressful work deadline — and the person says precisely the wrong thing, you erupt and say the words you would have stifled if your self-control strength was at full capacity. What do you call this process? My collaborators and I use the term “ego depletion” to refer to the state of depleted willpower. Initially, we called it “regulatory depletion” because the first findings focused purely on acts of self-regulation. When it emerged that the same resource was also used for decision-making, we wanted a broader term that would suggest some core aspect of the self was depleted. We borrowed the term “ego” from Freudian theory because Freud had spoken about the self as being partly composed of energy and of processes involving energy."
In his book, Baumeister explains that some people imagine that self-control or willpower is something you only use once in a while, such as when you are tempted to do something wrong. The opposite is true. Research indicates that the average person spends three to four hours a day resisting desires. Self-control is used for other things as well: controlling thoughts and emotions, regulating task performance and making decisions. Most people use their willpower many times a day, all day. And toward the end of the day, there is less gas in the tank.
We now know that people can improve their self-control even as adults. As with a muscle, it gets stronger from regular exercise. So engaging in some extra self-control activities for a couple weeks produces improvement in self-control, even on tasks that have no relation to the exercise activities. The exercises can be arbitrary, such as using your left hand instead of your right hand to open doors and brush your teeth. Or they can be meaningful, such as working to manage money better and save more. The important thing is to practice overriding habitual ways of doing things and exerting deliberate control over your actions. Over time, that practice improves self-control. As people deplete willpower, they became increasingly likely to give in to desires they might otherwise have resisted. This was true for all manner of desires: desires to sleep, to eat, to have sex, to play games, to spend money, to drink alcohol or smoke cigarettes.
One of the best features of Roy Baumeister's work, particularly his book on willpower, is that he is easy to read, accessible to those of us not trained in clinical research or adept at deciphering scientific papers.
Addictionary: Language of Addiction
For example, when the word "alcohol" was written or spoken in early 19th-century America. it was often used in the chemical and medical sense. This is from an article about drawing out the essence of stramonium, or jimson weed: "The virtues of stramonium," the New England Journal of Medicine reported in January of 1818, "appear to be seated in an extractive principle, which dissolves in water and alcohol."
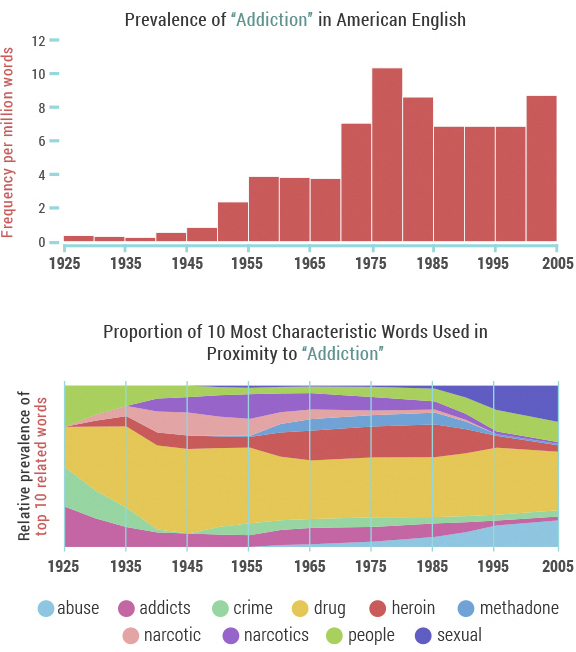
The word "cocaine" had different connotations as well. In the 1860s, for instance, a substance termed "cocaine" was advertised by a Boston company as a topical treatment to prevent hair loss.
Over time these words – "alcohol", "cocaine" and others, including "drugs" and" intoxicated" – became more closely associated with substance use, abuse and addiction in American popular culture.
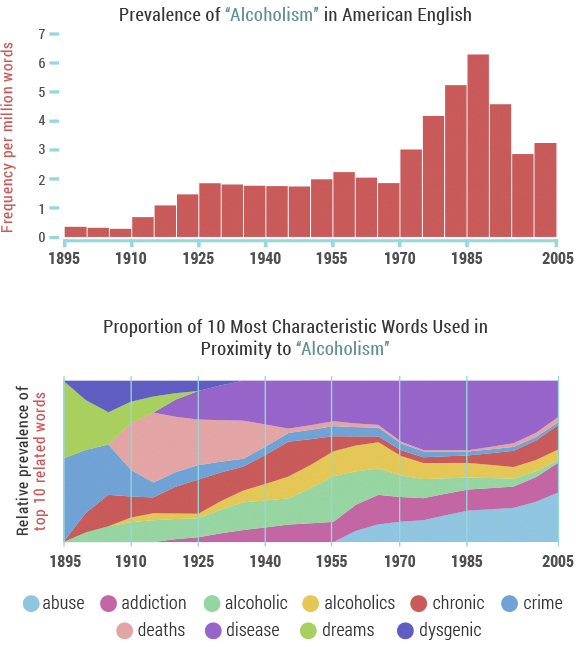
"'Alcoholism' made its debut in the lexicon around 1900, associated almost exclusively with 'crime' and 'dreams' – coincidentally around the time that Sigmund Freud's The Interpretation of Dreams was published," Recovery.org notes. "However, the association with crime was soon eclipsed by concern over 'chronic' alcoholism and 'death'/'deaths' related to alcoholism, which ballooned in the 1920s during the height of the prohibition movement." Documentarian Ken Burns echoes this in his series, Prohibition. One of the tragic unintended consequences of the nationwide crackdown on alcohol was an increase in dangerous, unregulated spirits — leading to 1,000 deaths a year.
Facebook, Twitter, and Linkedin
Videos Added to My Site
Genetics, Weird Facts, & Placebos
A placebo is anything that seems to be a "real" medical treatment -- but isn't. It could be a pill, a shot, or some other type of "fake" treatment. What all placebos have in common is that they do not contain an active substance meant to affect health. Younger physicians won't remember this, but years ago it was considered okay for doctors to prescribe placebos. Surgeons fairly often would substitute saline (salt water) injections when they worried that patients were asking for too many narcotic shots after an operation. There was a preparation called Gevrabon that was essentially sherry wine with some vitamins added, and it could be given by prescription "for relaxation at bedtime." Over the years, for obvious reasons, experts in medical ethics began to question whether these practices—essentially deceiving patients, but with good intentions—were proper and permissible.
In addiction medicine, I've seen college students come into the emergency room looking drunk, only to discover (with lab verification) that the "drug" they had tried was simply a vitamin pill. Similar findings have emerged at The University of Texas Austin, where one of the research labs has a full-fledged bar (i.e. a saloon) set up to simulate the settings where college students drink. Click here to see the Sahara Bar in the Department of Psychology. Study subjects sometimes get tipsy even when their margarita or manhattan contains no alcohol at all.
In 1996, scientists assembled a group of students and told them that they were going to take part in a study of a new painkiller, called "trivaricaine". Trivaricaine was a brown lotion to be painted on the skin, and smelled like a medicine. But the students were not told that, in fact, trivaricaine contained only water, iodine, and thyme oil – none of which are painkilling medicines. It was a fake – or placebo – painkiller. Read an abstract of the study: Mechanisms of Placebo Pain Reduction. With each student, the trivaricaine was painted on one index finger, and the other left untreated. In turn, each index finger was squeezed in a vice. The students reported significantly less pain in the treated finger, even though trivaricaine was a fake.
In this example, expectation and belief produced real results. The students expected the "medicine" to kill pain: and, sure enough, they experienced less pain. This is the placebo effect.
Placebo medicine has even been shown to cause stomach ulcers to heal faster than they otherwise would. These amazing results show that the placebo effect is real, and powerful. They mean that fake or placebo treatments can cause real improvements in health conditions: improvements we can see with our own eyes. Experiencing the placebo effect is not the same as being "tricked", or being foolish. The effect can happen to everyone, however intelligent, and whether they know about the placebo effect or not.
An article in Harvard Magazine describes Harvard Professor Dr.Ted Kaptchuk’s first randomized clinical drug trial, where nearly a third of his 270 subjects complained of awful side effects. All the patients had joined the study hoping to alleviate severe arm pain: carpal tunnel, tendinitis, chronic pain in the elbow, shoulder, wrist. In one part of the study, half the subjects received pain-reducing pills; the others were offered acupuncture treatments. And in both cases, people began to call in, saying they couldn’t get out of bed. The pills were making them sluggish, the needles caused swelling and redness; some patients’ pain ballooned to nightmarish levels. “The side effects were simply amazing,” Kaptchuk explains; curiously, they were exactly what patients had been warned their treatment might produce. But even more astounding, most of the other patients reported real relief, and those who received acupuncture felt even better than those on the anti-pain pill. These were exceptional findings: no one had ever proven that acupuncture worked better than painkillers. But Kaptchuk’s study didn’t prove it, either. The pills his team had given patients were actually made of cornstarch; the “acupuncture” needles were retractable shams that never pierced the skin. The study wasn’t aimed at comparing two treatments. It was designed to compare two fakes.
Dr. Kaptchuk and his colleagues have found that placebo treatments—interventions with no active drug ingredients—can stimulate real physiological responses, from changes in heart rate and blood pressure to chemical activity in the brain, in cases involving pain, depression, anxiety, fatigue, and even some symptoms of Parkinson’s. His work was also featured in a New Yorker article, "The Power of Nothing," that can be found here.
Here are four fascinating (and weird) facts about placebos and the placebo effect:
1. It doesn't have to be a secret. Some believe that a placebo can only work if the recipient is unaware they are taking one. But there's evidence that people with irritable bowel syndrome who knowingly receive a placebo do better than those who are left untreated.
2. It works better if it's expensive. The pain-killing power of a placebo pill is greater among people who are told they are taking a full-price version, compared to those told that the pill is on sale for a discounted price.
3. It's not just us, animals can get it too. A 2012 study found that between 30 and 40 per cent of rats experienced pain relief when their morphine injections were swapped for inactive saline solution.
4. It has an evil twin. The nocebo effect makes people undergoing treatment more likely to suffer from side-effects if they are warned about them by their doctor.
For the full New Scientist journal article on the subject, click here.
Slowly, over the past decade, researchers have begun to tease out the strands of the placebo response. The findings, while difficult to translate into medicine, have been compelling. In most cases, the larger the pill, the stronger the placebo effect. Two pills are better than one, and brand-name pills trump generics. Capsules are generally more effective than tablets, and injections produce a more pronounced effect than either. There is even evidence to suggest that the color of medicine influences the way one responds to it: colored pills are more likely to relieve pain than white pills; blue pills help people sleep better than red pills; and green capsules are the best bet when it comes to anxiety medication.
Mindfulness Based Relapse Prevention
Traditional treatment for substance abuse often focuses on avoiding or controlling triggers that result in negative emotion or craving. While research has shown that this approach can help, substance abuse relapse remains a problem: about half of those who seek treatment are using again within a year.
Bowen has spent much of her career studying another approach: mindfulness, which involves cultivating moment-to-moment, nonjudgmental awareness of thoughts, feelings, and surroundings. She and her colleagues have developed a program called Mindfulness-Based Relapse Prevention (MBRP), which combines practices like sitting meditation with standard relapse prevention skills, such as identifying events that trigger relapse. Rather than fighting or avoiding the difficult states of mind that arise when withdrawing from a substance, this combination tries to help participants to name and tolerate craving and negative emotion.
But how do mindfulness-based approaches compare to traditional substance abuse treatments? And do mindfulness-based treatments work for everyone? Researchers like Bowen are beginning to answer these questions.
Here is the key to the success of the program: MBRP helps people to relate differently to their thoughts, and use tools to disengage from automatic, addictive behaviors.
The JAMA Psychiatry article describes how effective the Mindfulness-Based Relapse Prevention program is in comparison to a standard relapse-prevention program as well as a conventional 12-step program. Six months following the intervention, the mindfulness-based program and the standard relapse-prevention program were both more successful at reducing relapse than the 12-step program. One year later, the mindfulness-based program proved better than the other two in reducing drinking and drug use.
Bowen says that when people cultivate mindfulness, they’re developing a tool to become aware of that inclination to want only pleasurable things and escape uncomfortable things. Mindfulness also helps people learn to relate to discomfort differently. When an uncomfortable feeling like a craving or anxiety arises, people like Sophia are able to recognize their discomfort, and observe it with presence and compassion, instead of automatically reaching for a drug to make it go away. Bowen says that awareness of our experience and the ability to relate to our experience with compassion gives us more freedom to choose how we respond to discomfort, rather than defaulting to automatic behaviors.
More research is needed to determine why MBRP might be more successful than other programs in reducing substance abuse relapse, but Bowen speculates that MBRP holds an advantage because mindfulness is a tool that can be applied to all aspects of one’s life.
Standard relapse-prevention programs teach tools specific to struggles with substance abuse—for instance, how to deal with cravings or how to say no when someone offers you drugs. A year after completing the program, a person may have a very different set of challenges that the relapse-prevention program did not equip them to deal with.
But because mindfulness is a tool that can be used in every part of a person’s life, practicing moment-to-moment awareness could continue to be an effective coping tool.
James Davis and his colleagues at Duke University are investigating mindfulness training as a way to help people quit smoking. Davis speculates that mindfulness is likely an effective tool in helping people with addiction because it’s a single, simple skill that a person can practice multiple times throughout their day, every day, regardless of the life challenges that arise. With so much opportunity for practice—rather than, say, only practicing when someone offers them a cigarette—people can learn that skill deeply.
Their intervention results showed a significant difference in smoking cessation for people who completed the intervention, as compared to people who were given nicotine patches and counseling from the Tobacco Quit Line.
Both Bowen and Davis emphasize that mindfulness is not a panacea; it doesn’t always work for everyone.
Dr. Zev Schuman-Olivier and his colleagues at the Massachusetts General Hospital Center for Addiction Medicine suggest that the type of therapy a person responds to may have something to do with their disposition. People who had the tendency to treat thoughts and behaviors with non-judgment and acceptance before the intervention began were more likely to be successful in reducing smoking following the mindfulness training. They write that if a person already has the skill to treat the self with non-judgment and acceptance, learning mindfulness practices likely comes easier to them than someone who has not previously practiced this skill.
Ultimately, the type of therapy that works best for a given person will likely capitalize on their pre-disposed strengths.Of course, as Bowen and Davis both note, the skills of mindfulness can be taught to everyone. But Schuman-Olivier’s finding suggests that people who are not oriented toward mindfulness may need a more vigorous or lengthy intervention, in order to more thoroughly learn mindfulness skills. It may be the case that people with less disposition toward mindfulness would fare better with a different therapy.
Another predictor of success in mindfulness-based treatment could be a person’s motivation to engage in the therapy. In Davis’ study, the people that started the intervention with the highest level of nicotine addiction were the most successful in reducing smoking by the end of the treatment. Davis said that this seemingly counterintuitive result likely reflects their motivation to quit; the people that were the most addicted had, at that point, tried everything, and were willing to try their hardest to make this therapy work. Meanwhile, people that were less addicted saw their addiction as less of a problem. They reasoned, “If this doesn’t work, I’ll be ok—something else will work, eventually.” As a result, they were likely less motivated to quit, and less engaged in the therapy.
Being Mindful and Positive
Mindfulness is natural, but we often overlook the importance of living in the present moment. There is not much new to learn; it's more about being aware of what is happening, who we are, and how to practice. We already have the capacity to be present, and it doesn’t require us to change who we are. You will hear me describe, in our conversations, topics like attention, awareness, empathy, compassion, being in the zone, situational awareness, presence, flow, contemplation, and many more. Being mindful has the power to change how we approach ourselves, our work, our relationships, and our communities. Mindfulness practice should be part of everyone's toolbox in the process of recovery from any mental or emotional setback. On my links page I have listed some useful resources on the subject.
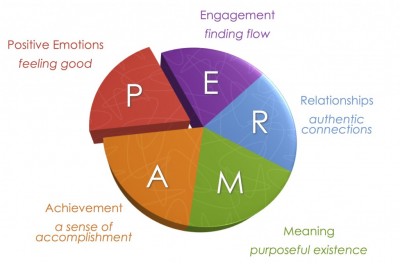
Positive psychology began to emerge in the late 1980's through the research of my colleague Dr. Martin Seligman. If you have attended my talks on the positive psychology of addiction recovery, you've heard me describe "PERMA," the five dimensions of life where positive psychology produces meaningful results. Seligman outlines the categories in his book, Authentic Happiness. The acronym for the five elements of Seligman’s well-being theory is PERMA (Positive Emotions, Engagement, Relationships, Meaning and purpose, and Accomplishments).
What people in addiction recovery notice, usually right away, is the strong similarity between the findings of positive psychology research and the guiding principles of twelve step recovery.
Positive emotions include a wide range of feelings, not just happiness and joy. Included are emotions like excitement, satisfaction, pride and awe, amongst others. These emotions are frequently seen as connected to positive outcomes, such as longer life and healthier social relationships.
Engagement refers to involvement in activities that draws and builds upon one’s interests. Mihaly Csikszentmihalyi explains true engagement as flow, a feeling of intensity that leads to a sense of ecstasy and clarity. The task being done needs to call upon higher skill and be a bit difficult and challenging yet still possible. Engagement involves passion for and concentration on the task at hand and is assessed subjectively as to whether the person engaged was completely absorbed, losing self-consciousness.
Relationships are all important in fueling positive emotions, whether they are work-related, familial, romantic, or platonic. We receive, share, and spread positivity to others through relationships. They are important in not only in bad times, but good times as well. In fact, relationships can be strengthened by reacting to one another positively. It is typical that most positive things take place in the presence of other people.
Meaning is also known as purpose, and prompts the question of “Why?” Discovering and figuring out a clear “why” puts everything into context from work to relationships to other parts of life. Finding meaning is learning that there is something greater than you. Despite potential challenges, working with meaning drives people to continue striving for a desirable goal. The three criteria are that it 1) contributes to well-being, 2) is pursued for its own sake, and 3) is measured independently of the other elements of PERMA.
Accomplishments are the pursuit of success and mastery. Unlike the other parts of PERMA, they are sometimes pursued even when it does not result in positive emotions, meaning, or relationships. Accomplishment can activate the other elements of PERMA, such as pride under positive emotion.Accomplishments can be individual or community based, fun or work based.
The five domains are valuable to consider when "the program isn't working," because taking personal inventory usually comes down to looking at what's going on inside these categories. The five elements were sifted out of research on thousands of individuals who were interviewed on the broad topic of happiness.
Change Your Brain
BRAINHEALTH PHYSICALS
A unique cognitive assessment that measures cognitive reserve in pivotal areas of higher-order mental functioning, all of which rely on robust frontal lobe function. It is just as essential to measure and monitor brain fitness as it is to measure and monitor physical fitness. Get a benchmark of your brain’s health.
HIGH PERFORMANCE BRAIN TRAINING
The high performance brain training program, Strategic Memory Advanced Reasoning Training (SMART®
I joined the staff at The Center for BrainHealth and BPI after extensive contact with the scientists and clinicians there. Over a period of months I found myself returning at least once or twice weekly to attend a lecture, to discuss research, or to interact with my friends on The Warrior Team, a powerful resource for veterans. I remember the day in November 2014 when I spoke with Dr. Sandra Chapman, the CEO, and she asked me whether I was enjoying my visits. "Are you kidding me?" I said, "I want to be more than a visitor—I want to work here!" Needless to say, I was both honored and extremely delighted when, early in 2015, I got the call and the invitation to be Senior Medical Advisor for CBH and BPI.
Brain Scams: Don't Buy the MRI
Dr. Carlat writes: "My journey through the land of functional neuroimaging has helped me to understand how spectacularly meaningless these images are likely to be. Most neuromarketers are using these scans as a way of sprinkling glitter over their products, so that customers will be persuaded that the pictures are giving them a deeper understanding of their mind. In fact, imaging technologies are still in their infancy. And while overenthusiastic practitioners may try to leapfrog over the science, real progress, which will take decades, will be made by patient and methodical researchers, not by entrepreneurs looking to make a buck."
If a person has a brain tumor, a brain aneurysm, or a stroke, then brain imaging can be helpful. However, brain imaging makes no difference (and makes no sense) in the treatment of problems like depression, anxiety, ADD/ADHD, alcoholism, addictions, or other commonly seen psychiatric disorders.
Brain imaging is very expensive, and the brain is exposed to radiation during a scan. This is an unnecessary risk, and a very expensive procedure, for anyone with a psychiatric disorder.
Beliefs Shape Our Reality
Surprisingly large numbers of people also hold beliefs that a psychiatrist would class as delusional. In 2011, psychologist Peter Halligan at Cardiff University assessed how common such beliefs were in the UK (see below for the top 10 delusions). He found that more than 90 per cent of people held at least one, to some extent. They included the belief that a celebrity is secretly in love with you, that you are not in control of some of your actions, and that people say or do things that contain special messages for you (Psychopathology, vol 44, p 106).
None of Halligan's subjects were troubled by their strange beliefs. Nonetheless, the fact that they are so common suggests that the "feeling of rightness" that accompanies belief is not always a reliable guide to reality.
The Top 10 Delusions
1. Your body, or part of your body, is misshapen or ugly 46.4%
2. You are not in control of some of your actions 44.3%
3. You are an exceptionally gifted person that others do not recognise 40.5%
4. Certain places are duplicated, i.e. are in two different locations at the same time 38.7%
5. People say or do things that contain special messages for you 38.5%
6. Certain people are out to harm or discredit you 33.8%
7. Your thoughts are not fully under your control 33.6%
8. There is another person who looks and acts like you 32.7%
9. Some people are duplicated, i.e. are in two places at the same time 26.2%
10. People you know disguise themselves as others to manipulate or influence you 24.9%
One of the most interesting things about belief is that it varies enormously from person to person, especially on issues that really matter such as politics and religion. According to research by Gerard Saucier of the University of Oregon, these myriad differences can be boiled down to five basic "dimensions" (Journal of Personality and Social Psychology, vol 104, p 921). At their core, he says, these concern what we consider to be worthy sources of value and goodness in life, whether it be a concept, an object, a supernatural being or a historical person. Your belief system is the aggregate of your position on each of these five dimensions, which are independent of each other.
1. Traditional religiousness: level of belief in mainstream theological systems such as Christianity and Islam
2. Subjective spirituality: level of belief in non-material phenomena such as spirits, astrology and the paranormal
3. Unmitigated self-interest: belief in the idea that hedonism is a source of value and goodness in life
4. Communal rationalism: belief in the importance of common institutions and the exercise of reason
5. Inequality aversion: level of tolerance of inequality in society, a proxy of the traditional left-right political split
To read the full article, click here.
Changing the Brain
People with chronic fatigue syndrome (CFS) tend to have a decrease in a type of brain tissue called grey matter in the prefrontal cortex of the brain. OCD researchers in the Netherlands provided 16 sessions of CBT, and found significant increases in gray matter volume in the prefrontal cortex. This seems to suggest that the CFS patients were able to “recover” some gray matter volume after CBT.
The bottom line: Although medication and psychotherapy appear to work their magic in difference places, the results are positive for both. The mechanism of action remains unclear, but studies also show that the combination of psychotherapy and the right medication (getting it right is very important!) is an excellent approach for many individuals. As the brain changes, we see the production of new proteins, which change our brains through neuroplasticity. In selecting a treatment strategy, sometimes medication works best, sometimes psychotherapy is the best option, and sometimes it’s a combination of the two.
What Is a Disease?
The ancient Greek academies had differing views of disease. Hippocrates emphasized the sick individual with his particular kind of misery. Others saw disease as a specific pathological process, evidenced by a visible sign such as a tumor, wound, or physical symptom. To this day, the definition of disease remains controversial. The AMA Council on Science and Public Health recently addressed the question, “Is obesity a disease?” The Council’s response: “Without a single, clear, authoritative, and widely accepted definition of disease, it is difficult to determine conclusively whether or not obesity is a medical disease state.”
This is also true for the vast majority of psychiatric disorders, particularly the addictions. The individual’s degree of suffering and incapacity—or distress and dysfunction—defines a state of disease. Although we now have some clues about the causes of mental disorders, and neuroimaging studies are making great strides, the American Psychiatric Association takes this position:
“The exact causes of mental disorders are unknown, but an explosive growth of research has brought us closer to the answers. We can say that certain inherited dispositions interact with triggering environmental factors. Poverty and stress are well-known to be bad for your health—this is true for mental health and physical health. In fact, the distinction between “mental” illness and “physical” illness can be misleading. Like physical illnesses, mental disorders can have a biological nature. Many physical illnesses can also have a strong emotional component.”
The National Alliance on Mental Illness (NAMI) seems to agree: “A mental illness is a condition that impacts a person's thinking, feeling or mood may affect and his or her ability to relate to others and function on a daily basis. Each person will have different experiences, even people with the same diagnosis. Recovery, including meaningful roles in social life, school and work, is possible, especially when you start treatment early and play a strong role in your own recovery process. A mental health condition isn’t the result of one event. Research suggests multiple, interlinking causes. Genetics, environment and lifestyle combine to influence whether someone develops a mental health condition. A stressful job or home life makes some people more susceptible, as do traumatic life events like being the victim of a crime. Biochemical processes and circuits as well as basic brain structure may play a role too.”
These questions highlight the importance of seeing the suffering person as more than a diagnosis or a label. This is the message I emphasize in my presentation, “Four Sides to Every Story,” available on request. Diagnosis is helpful, because we know that certain treatments are effective for certain diseases. For example, some fevers are caused by infection, and if we kill the offending bug we can cure the disease. Other fevers are caused by inflammation—as in rheumatoid arthritis or drug reactions—and if we calm the inflammation we can ease the fever.
At the same time, the psychiatrist should see much more than a label or a diagnosis (what the patient has in terms of the disease model). The psychiatrist—or any mental health professional—should also take the other three perspectives into account: who the person is, what the person does, and what the person has encountered. Using all four perspectives, the disease model can be valuable. It’s just not the whole story.
Painkillers, Narcotic Abuse, and Addiction
Over the past twenty years, drugs like hydrocodone, oxycontin, and similar narcotics have become an epidemic problem.
Opioids -- also called opiates or narcotics -- are pain relievers made from opium, which comes from the poppy plant. Morphine and codeine are the two natural products of opium. Synthetic modifications or imitations of morphine produce the other opioids:
Heroin (street drug)
Dilaudid (hydromorphone)
Percocet, Percodan, OxyContin (oxycodone)
Vicodin, Lorcet, Lortab (hydrocodone)
Demerol (pethidine)
Methadone
Duragesic (fentanyl)
When people use narcotics only to control pain, they are unlikely to become addicted to the drugs. However, opioids provide an intoxicating high when injected or taken orally in high doses. Opioids are also powerful anxiety relievers. For these reasons, narcotic abuse is one of the most common forms of drug abuse in the U.S.
Terms like opioid abuse, drug abuse, drug dependence, and drug addiction are often used interchangeably, but experts define them as follows:
Drug abuse, including opioid abuse, is the deliberate use of a medicine beyond a doctor's prescription. In the case of opiates, the intention is generally to get high or to relieve anxiety.
Dependence occurs when the body develops tolerance to the drug, meaning higher doses are needed for the same effect. In addition, stopping the drug produces drug withdrawal symptoms.
Drug addiction occurs when the person has drug dependence, but also displays psychological effects. These include compulsive behavior to get the drug; craving for the drug; and continued use despite negative consequences, like legal problems or losing a job.
Symptoms of Narcotic Abuse
Signs and symptoms of opioid abuse include:
- Analgesia (feeling no pain)
- Sedation
- Euphoria (feeling high)
- Respiratory depression (shallow or slow breathing)
- Small pupils
- Nausea, vomiting
- Itching or flushed skin
- Constipation
- Slurred speech
- Confusion or poor judgment
Symptoms of Opioid Drug Withdrawal
If a person uses opioids for a long time, they develop physical dependence and tolerance. Usually, opioid abusers will then take more of the drug, to continue to get high. If a person stops using opioids after they become physically dependent on the drug, they will experience drug withdrawal symptoms which can include:
Anxiety
Irritability
Craving for the drug
Rapid breathing
Yawning
Runny nose
Salivation
Gooseflesh
Nasal stuffiness
Muscle aches
Vomiting
Abdominal cramping
Diarrhea
Sweating
Confusion
Enlarged pupils
Tremors
Loss of appetite
I tell patients that withdrawal from drugs like painkillers and heroin is like the worst case of the flu you've ever experienced. The symptoms of opioid drug withdrawal can be agonizing and intolerable, contributing to continued drug abuse. In general, how severe opioid drug withdrawal symptoms are, and how long they last, depends on how long the person has been abusing opioids and how much they have been taking.
Medicines like methadone, buprenorphine (sometimes combined with naloxone), and naltrexone can be taken in various forms and are used to prevent withdrawal symptoms after a person stops using, a process called detoxification ("detox"). After drug withdrawal is complete, the person is no longer physically dependent on the drug. But psychological dependence can continue. Some people with drug addiction may relapse in response to stress or other powerful triggers.
Dependence vs. Addiction
Controlling pain is the goal when opioids are used medically. Patients or health care professionals should not let fear of addiction prevent them from using opioids for effective pain relief. Knowing the difference between dependence and addiction is important.
People who take opioids for pain relief for extended periods of time may need higher doses to ease their pain. They may develop tolerance to the drug and experience withdrawal symptoms if the medication is abruptly stopped. They become physically dependent on the drug.
Addiction occurs when narcotic abuse becomes compulsive and self-destructive, especially concerning an opioid user's need to use the drug for reasons other than pain relief.
To prevent withdrawal symptoms in people who have become physically dependent on opioids for pain relief, the dose may be slowly lowered over a few weeks. People who are weaned off opioids and are pain free usually don't start taking the drug again or become abusers of narcotics. Opioids used for short-term medical conditions rarely require weaning. In those cases, stopping the medication after a brief period usually doesn't cause withdrawal symptoms.
Other Abused Drugs
Strictly speaking, most drugs referred to informally as narcotics really aren't. However, two drug classes have some similar effects to opioids, when abused:
Benzodiazepines include Valium, Ativan, and Xanax. Benzodiazepine abuse results in sedation and calm, but tolerance develops rapidly. Withdrawal can result in seizures, unlike opioid withdrawal.
Barbiturates include Seconal, Amytal, Nembutal, and Luminal. Barbiturates are also sedating and calming. Withdrawal after continued barbiturate abuse, like benzodiazepine abuse, is medically serious.
In general, benzodiazepines and barbiturates have less pain-relieving effects than opioids. All three drug classes are sedating and anxiety-relieving. Benzodiazepine abuse, barbiturate abuse, and narcotic abuse all produce tolerance and physical dependence over time, and withdrawal symptoms after sudden discontinuation.
This post includes material from WebMD Medical Reference.
SOURCES:
Van den Brink, W. Canadian Journal of Psychiatry, 2006.
WebMD Medical Reference: "Narcotic Abuse."
Bateson, A.N. Current Pharmaceutical Design, January 2002.
eMedicine.com: "Toxicity, Barbiturate."
Reviewed by Arefa Cassoobhoy, MD, MPH on August 01, 2013
Science on Will and Willpower - Part I
We are the only sentient creatures having the capacity to know our own will and assert our will. Frankfurt also observes, in his elegant essays, that human beings are uniquely capable of knowing that there are times when "the will that I have is not the will that I want to have." For example, someone may want to learn to play the piano, but they may say, "I can't find the will to practice." They want to have the will to practice, but somehow it's not there, or it's subordinated to a different expression of will. The same is often true of addicts and alcoholics. Wanting to stay sober, the alcoholic/addict yearns for "the will to stay sober," but often the search for the will comes up empty. Alcoholics Anonymous teaches that alcoholics cannot will themselves to quit drinking—indeed, that self-will and self-centeredness are likely a root cause of the drinking. Yet recovering addicts must be willing. That is, they must be open to the possibility that the group and its principles are powerful enough to trump a compulsive disease.
For decades Frankfurt's scholarship failed to receive the attention it deserved, and then neuroscience became an unexpected ally in the philosophical inquiry. At the University of Illinois, for example, Dr. Ibrahim Senay has studied the concepts of will and willingness from the perspective of clinical psychology. Senay figured out an intriguing way to explore possible connections among will, willingness, intention, motivation and goal-directed actions. In short, he identified some key traits needed to achieve any personal objective, from losing weight to learning to play play piano.
Senay did this by exploring self-talk. Self-talk is just what it sounds like—that voice in your head that articulates what you are thinking, spelling out your options and intentions and hopes and fears, and so forth. It is the ongoing conversation you have with yourself. Senay thought that the form and texture of self-talk—right down to the sentence structure—might be important in shaping plans and actions. What’s more, self-talk might be a tool for exerting the will—or experiencing willingness.
Senay's study involved two groups. One of the groups was told that they might be working on a task (solving a puzzle), and the other group was told that they actually would be working on a task. The first group was instructed to think about whether they would, or would not, be asked to work the puzzles. The second group was told that in a few minutes they would definitely be doing the puzzles. In this clever way, Senay created one group contemplating the question, "Will I be doing this?", and another group thinking, "I will be doing this," declaring their objective to themselves.
As it turned out, people with wondering minds (contemplating what might possibly happen) completed significantly more puzzles than did those with willful minds (thinking what they definitely were about to do). In other words, the people who kept their minds open were more goal-directed and more motivated than those who declared their objective to themselves.
The point is that questions, by their nature, speak to possibility and freedom of choice. Meditating on them might enhance feelings of autonomy and intrinsic motivation, creating a mind-set that promotes success. There is a scientifically verifiable difference between asking, and contemplating, the question "Will I?" versus narrowing the focus to a willful, determined statement, "I will."
What’s more, when the volunteers were questioned about why they felt they would be newly motivated to get to the gym more often, those primed with the question said things like: “Because I want to take more responsibility for my own health.” Those primed with “I will” offered strikingly different explanations, such as: “Because I would feel guilty or ashamed of myself if I did not.”
According to Wray Herbert, who summarized the research in Scientific American magazine, "This last finding is crucial. It indicates that those with questioning minds were more intrinsically motivated to change. They were looking for a positive inspiration from within, rather than attempting to hold themselves to a rigid standard." And there was more: "Those asserting will lacked this internal inspiration, which explains in part their weak commitment to future change. Put in terms of addiction recovery and self-improvement in general, those who were asserting their willpower were in effect closing their minds and narrowing their view of their future. Those who were questioning and wondering were open-minded—and therefore willing to see new possibilities for the days ahead."
In terms of Professor Frankfurt's metaphysical philosophy, the individual who thinks about his will and asks, "Will I?" opens the door to possibility and freedom of choice. The key to satisfaction, Frankfurt says, is "taking ourselves seriously, and getting it right."
In terms of Alcoholics Anonymous, the person who seeks to exercise willpower and "an iron will with grim determination" is much less likely to succeed. The person who struggles with AA is the person who says, "I know what I need to do, and now I just need to do it." The more successful person asks, "If I knew what I need to do, I probably would have done it by now, so I wonder what I will do?"
Do 12-Step Programs Work?
Since the 1930's when Bill W. and Dr. Bob started Alcoholics Anonymous (AA) the fellowship has grown to over two million members. Meeting in rented rooms, school halls, hospitals, and the storied church basement, AA and similar 12-step organizations (eg, Narcotics Anonymous [NA]) remain the most commonly sought sources of help for substance-related problems in the United States (Substance Abuse and Mental Health Services Administration. Results from the 2007 National Survey on Drug Use and Health: National Findings. Rockville, MD: Office of Applied Studies; 2008).
Research has shown that attending AA, either alone or during and following professional treatment, enhances outcomes. One naturalistic study, for example, followed 466 previously untreated individuals with problem drinking for eight years. Participants self-selected into one of four groups: no treatment, AA alone, formal treatment alone, and formal treatment plus AA. Those who received some sort of help—AA, formal treatment, or both—had higher rates of abstinence at all time points. At eight years, 26% of patients in the no treatment group were abstinent from alcohol compared to 49% who received AA alone, 46% who received formal treatment alone, and 58% who received the combination of treatment plus AA (Timko C et al, J Stud Alcohol 2000;61(4):529–540).
A systematic Cochrane review of the best scientific studies on AA and TSF found that they were as effective as any of the interventions to which they were compared for some factors, such as retention in treatment, but found that no studies unequivocally proved AA and TSF were superior to other treatments (Ferri M et al, Cochrane Database Syst Rev 2006;(3):CD005032).
Other studies have found a linear dose-response relationship between AA attendance and favorable drinking outcomes (Kaskutas LA, J Addict Dis 2009;28(2):145–157). Attending one meeting per week, on average, appears to be the minimum threshold to realize benefit and increasing meeting frequency is associated with progressively greater rates of abstinence. In addition, research has shown that women engage with AA as much as men, become more involved with the 12 Steps, and derive similar benefit. In 1990, the Institute of Medicine called for more research on how AA works. Since then, research has revealed that AA aids recovery through multiple mechanisms, many of which are also activated by professional behavioral treatments (Kelly J et al, Addict Res Theory 2009:17(3):236–259).
Most consistently and strongly, AA appears to work by helping people make positive changes in their social networks (eg, by dropping heavy drinkers/drug users and increasing abstainers/low risk drinkers), and by enhancing coping skills and self-efficacy for abstinence when encountering high-risk social situations (see for example, Kelly JF et al, Drug Alcohol Depend 2011;114(2–3):119–126).
Among more severely addicted people, AA also appears to work by enhancing spiritual practices, reducing depression, and increasing individuals’ confidence in their ability to cope with negative emotion (Kelly JF et al, Addiction 2012;107(2)289–299). Thus, AA appears to work through diverse mechanisms and may work differently for different people. Stated another way: individuals may use AA differently, depending on their unique needs and challenges.
Research has shown that involvement in 12-step work can reduce the need for more costly treatments while simultaneously improving outcomes. A large multicenter study of over 1,700 patients found those treated in professional 12-step treatment went on to participate in community-based AA and NA meetings at a higher rate than those from professional cognitive behavioral therapy (CBT) programs, who relied more heavily on professional services. This translated into a two-year savings of over $8,000 per patient among 12-step treated patients, without compromising outcomes. In fact, those treated in the 12-step treatment programs had one-third higher rates of abstinence across follow-up (Humphreys K & Moos R, Clin Exp Res 2001;25(5):711–716; Humphreys & Moos, Alcohol Clin Exp Res 2007;31(1):64–68).
Project MATCH was a large randomized trial comparing three individually-delivered psychosocial treatments for alcohol use disorder—TSF, CBT, and Motivational Enhancement Therapy (MET)—that was funded by NIAAA. It included 1,726 patients from nine clinical sites across the US (Project Match Research Group, J Stud Alcohol 1997;58(1):7–29). TSF was found to be as effective as the more empirically supported CBT and MET interventions at reducing the quantity and frequency of alcohol use post-treatment and at one- and three-year follow-ups. Moreover, TSF was superior to CBT and MET at increasing rates of continuous abstinence, such that 24 percent of the outpatients in the TSF condition were continuously abstinent at one year after treatment, compared with 15 percent and 14 percent in CBT and MET, respectively (Tonigan JS et al,Participation and involvement in Alcoholics Anonymous. In: Babor TF & Del Boca FK, eds. Treatment Matching in Alcoholism. New York: Cambridge University Press;2003:184–204).
Abstinence rates at three years continued to favor TSF, with 36 percet reporting complete abstinence, compared with 24 percent in CBT, and 27 percent in MET (Cooney N et al. Clinical and scientific implications of Project MATCH. In: Babor TF & Del Boca FK, eds. Treatment Matching in Alcoholism. New York: Cambridge University Press; 2003:222–237).
In light of findings from several such RCTs that demonstrated the efficacy of TSF, this therapy was added to the Substance Abuse and Mental Health Services Administration’s (SAMHSA) National Registry of Evidence-Based Practices and Programs (NREPP) in 2008.
The overwhelming majority of research has been conducted on AA. More research is needed on other MHOs, such as SMART Recovery, LifeRing, Celebrate Recovery, Women for Sobriety, Moderation Management, and others, so that more objective evidence is gathered on secular, religious, and non-abstinence-based AA alternatives (see the article "Alternatives to 12-Step Recovery" for more on these groups).
Identifying the Effective Psychiatrist
Practicing medicine is a privilege granted to very few individuals, and I am indeed fortunate. Within the field of medicine, working in psychiatry requires more than an understanding of anatomy and organ systems, because psychiatry is about the mind, the brain, the self, and human experience.
Like any other professional, I believe in high ethical standards, sound knowledge of my field, and the importance of practicing wisely and compassionately. Beyond the obvious nostrums and philosophical cliches, however, I want to be one of the good psychiatrists. As I thought about this lately, I began to wonder: how does one identify and recognize a really good psychiatrist? What makes a good psychiatrist? If I made a list of the most important aspects of a psychiatrist’s professional philosophy, what would that look like?
In 2006 an article was published in the Journal of Affective Disorders showing that good psychiatrists prescribing placebos (sugar pills) had better results than poor psychiatrists prescribing actual medication. Over 120 patients were divided into two groups, one group that received sugar pills and another group that received full strength psychiatric medication for depression. At the same time, each psychiatrist was rated on a number personal qualities: verbal fluency, interpersonal perception, expressiveness, warmth, acceptance, empathy, and the ability to focus on the other person. When results were analyzed, the psychiatrists strong in these personal qualities had the best results, even when the “medication” they prescribed was not medication at all.
The effective psychiatrists were fluent, clear, and expressive in speaking, and they had an accurate feel for their patients. Rather than being distant and aloof, the good psychiatrists were warm, friendly, and accepting. The good psychiatrists empathized well, spent more time with their patients, were more thoughtful in their strategies, and formed strong therapeutic partnerships. The point of the study was that having a good psychiatrist makes a difference in recovery.
Although medication can be extremely helpful in psychiatric care, treatment is not all about medication. The combination of the right medication, the right psychotherapy, and the right psychiatrist is the key to success.
Research has shown for generations that some clinicians consistently produce better results than others, regardless of the type of psychotherapy or theoretical orientation of the practitioner. Hundreds of studies have shown that the differences between types of psychotherapy is very small, but the psychiatrist providing the psychotherapy is critically important.
Over the past fifteen years, extensive research has given us a solid body of evidence about the qualities and actions of effective psychiatrists. Based on the psychotherapy research of Dr. Bruce Wampold of The University of Wisconsin, I have formulated here an inventory that provides the basis for judging whether a psychiatrist is likely to be effective.
- Effective psychiatrists demonstrate a sophisticated set of interpersonal skills, including verbal fluency, perceptiveness of others, emotional intelligence, expressiveness, warmth, and acceptance. Given these gifts, the most effective psychiatrists are those who are first excellent physicians, well trained in medicine, competent to practice at the highest levels.
- Effective psychiatrists are inquisitive, questioning, and seeking new knowledge constantly. They embrace science while at the same time possessing the humility to know how little we really know.
- Patients of effective psychiatrists feel understood, trust the psychiatrist, and believe the psychiatrist can help. The psychiatrist creates these conditions in the first moments in both speech and action. In the initial contacts, patients are very sensitive to cues of acceptance, understanding, and expertise. Although these conditions are necessary throughout therapy, they are most critical in the initial interaction to ensure engagement in the therapeutic process.
- Effective psychiatrists are able to form a working alliance with a broad range of patients. The working alliance involves the therapeutic bond, but also importantly agreement about the task of goals of therapy. The working alliance is described as collaborative, purposeful work on the part of the patient and the psychiatrist. The effective psychiatrist builds on the patient’s initial trust and belief to form this alliance and the alliance becomes solidly established early in therapy.
- Effective psychiatrists provide an acceptable and practical explanation for the patient’s distress. The patient wants an explanation for his or her symptoms or problems. There are several considerations involved in providing the explanation. First, the explanation must be consistent with the healing practice. On the medical side, the explanation is biological, and in psychotherapy the explanation is psychological. Second, the explanation must be acceptable and compatible with the patient’s attitudes, values, culture, and worldview. Third, the explanation must provide a strategy by which the patient can overcome difficulties and solve life’s problems. These three factors together make for a strong therapeutic alliance.
- The effective psychiatrist provides a treatment plan that is consistent with the explanation provided to the patient. Once the patient accepts the explanation, the treatment plan will make sense and patient compliance will be increased. The treatment plan must involve healthy actions—the effective psychiatrist promotes healing by replacing failed strategies with effective strategies. At the same time, strong defenses will replace weak defenses, and healthy practices will replace self-defeating behaviors.
- The effective psychiatrist is influential, persuasive, and convincing. The psychiatrist presents the explanation and the treatment plan in a way that convinces the patient that the explanation is correct and that following through with the treatment will benefit the patient. This process leads to patient hopefulness, increased expectancy for mastery, and healthy actions. These characteristics are essential for forming a strong working alliance.
- The effective psychiatrist is honest and authentic. Authenticity refers to communication to the patient that the psychiatrist truly wants to know how the patient is doing. The best psychiatrists tend not to use checklists, scales, and paper measures. Instead, they talk and listen openly and honestly.
- The effective psychiatrist is flexible and will be patient if resistance to the treatment is apparent or the patient is slow to make progress. Although the effective psychiatrist is persuasive, persuasion can be a process that takes time. The good psychiatrist pays attention, takes in new information, test hypotheses about the patient, and is willing to be wrong. A good psychiatrist will seek second opinions, refer to other specialists, and even take calculated risks such as trying a new approach or a newly released medication.
- The effective psychiatrist does not avoid difficult material in therapy. Doctor and patient must use such difficulties therapeutically. We all tend to avoid material that is difficult. The effective psychiatrist senses avoidance is taking place and does not collude to avoid the material. Instead, the psychiatrist will discuss the difficult material and address difficult problems. Sometimes conversations can be difficult, and at times the relationship between doctor and patient can be strained, but this is part of the work of therapy. The good psychiatrist can use skill, experience, and compassion to overcome these barriers to recovery.
- The effective psychiatrist communicates hope and optimism. Sometimes this is easy to do, and sometimes it’s difficult. The working partnership must maintain hope and optimism in the face of chronic illness, relapses, lack of consistent progress, and many other difficulties. Effective psychiatrists acknowledge these issues and still communicate hope that the patient will achieve realistic goals in the long run. This communication is not blind faith or Pollyanna optimism, but rather a firm belief that together the psychiatrist and patient will work successfully. At the same time, effective psychiatrists mobilize patient strengths and resources to facilitate the patient’s ability to solve his or her own problems. The best doctors know that the patient, through his or her work, is responsible for therapeutic progress, creating a sense of mastery.
- Effective psychiatrists are aware of the patient’s characteristics and context. This is a tall order with many categories: culture, race, ethnicity, spirituality, sexual orientation, age, physical health, motivation for change, and beyond. Furthermore, the effective psychiatrist is aware of how his own background, personality, and beliefs figure into the relationship.
- The effective psychiatrist is aware of his or her own psychological process and does not inject his or her own material into the therapy process unless such actions are deliberate and therapeutic.
- The effective psychiatrist is aware of the best research evidence related to the particular patient, in terms of treatment, problems, and social context. It is very important to understand the biological, social, and psychological basis of the patient’s problem.
- The effective psychiatrist seeks always to improve, always to be a student. Hippocrates said, “The life so short, the craft so long to learn,” and truer words were never spoken.
- Finally, the good psychiatrist must possess both humility and a sense of humor. We will never know enough, or be wise enough, to have all the answers. We cannot take ourselves too seriously, lest we become arrogant, prideful, and set ourselves apart from those who have graced us with the privilege of being socially sanctioned healers.
Development of skill in psychiatry involves intensive practice and unceasing professional growth. Patients are sometimes our best and most effective teachers. A few years ago I taught a seminar for third year students at the University of Texas Southwestern Medical School, “Psychiatric Nightmares, Disasters, and Catastrophes.” The entire content of the seminar consisted of mistakes I’d made, errors I had committed, and pitfalls that these students likely would encounter, sooner or later, in their medical careers.
I told the story of a patient with whom I’d had a terrible, angry argument, and how guilty I felt for years about my lack of composure—only to have the patient return, two years later, to ask me for a job at the hospital and tell me that she had been shaken into reality by our confrontation. I told them the story of the patient who overdosed and came to the ICU, and how I was baffled by the case—until I realized that the patient had diabetes, and was actually in a diabetic coma, not a drug-induced state.
I told them about the patient who came to the doorstep of my home on a Sunday afternoon, bearing in her arms her injured pet cat, hoping that I could help. I told them about an elderly man from New Orleans who was my patient in the middle of the night as Hurricane Katrina washed away his home.
And I told them about the time when I was called to the ER to examine a beautiful young woman, a Duke University cheerleader, who had bruised her shoulder. When I approached her to examine the injury, and she undid her gown and dropped it with a smile, I calmly reached into the pocket of my white coat for my stethoscope, only to realize that I then stuck my reflex hammer in my ear.
These encounters are the building blocks of the effective psychiatrist’s life. I’ve come to realize that most of the learning happens after we graduate. As Dr. Stead used to say at Duke, “Medical school is where you stay for four years until you’re old enough to become a doctor.”
Neuroscience of Belief
In 1921, philosopher Bertrand Russell put it succinctly when he described belief as "the central problem in the analysis of mind". Believing, he said, is "the most 'mental' thing we do" – by which he meant the most removed from the "mere matter" that our brains are made of. How can a physical object like a human brain believe things? Philosophy has made little progress on Russell's central problem. But increasingly, scientists are stepping in.
The neuroscientific investigation of belief began in 2008, when Sam Harris (Harris, S., Sheth, S. A. and Cohen, M. S. (2008), Functional neuroimaging of belief, disbelief, and uncertainty. Ann Neurol., 63: 141–147) at the University of California, Los Angeles, put people into a brain scanner and asked them whether they believed in various written statements. Some were simple factual propositions, such as "California is larger than Rhode Island"; others were matters of personal belief, such as "There is probably no God". Harris found that statements people believed to be true produced little characteristic brain activity – just a few brief flickers in regions associated with reasoning and emotional reward. In contrast, disbelief produced longer and stronger activation in regions associated with deliberation and decision-making, as if the brain had to work harder to reach a state of disbelief. Statements the volunteers did not believe also activated regions associated with emotion, but in this case pain and disgust.
To read the full article, click here.
Two Talks Today to Good Teams
Be a Better Spouse or Partner
#1 Be nice as often as you can.
A lot of modern relationship therapy is based on the research of John Gottman, a prolific psychologist famous for videotaping thousands of couples and dissecting their interactions into quantifiable data. One of his most concrete findings was that happier couples had a ratio of five positive interactions to every negative interaction. “That just leapt off the pages of the data analysis,” he says. It was true in very different types of relationships, including those in which the people were very independent and even distant or argumentative. These positive interactions don't have to be grand gestures: “A smile, a head nod, even just grunting to show you're listening to your partner—those are all positive,” Gottman says.
#2 Think about what your partner needs, even when fighting.
To resolve conflicts, Gottman says we can learn from game theory—the study of conflict and decision making used in political science, sociology and economics. It used to be widely accepted that negotiations were mostly zero-sum situations, meaning one party's gain was the other party's loss. In 1950 mathematician John Nash proved there was another, better outcome: a solution in which the parties may have to compromise, but in the end all of them come out satisfied. (This now famous “Nash equilibrium” won him a Nobel Prize in 1994.) I'm reminded of a recent situation in my own marriage—my husband hated the house we bought a couple of years ago and wanted to move to a different neighborhood; I liked the house just fine and didn't want to goanywhere. After much discussion, we realized that what we both really want is to settle in somewhere for the long haul. If the current house is not a place my husband feels he can settle in, then I can't truly settle in either. So we're moving next month, for both our sakes! Find the Nash equilibrium in your conflict, and you'll both get your needs met.
#3 Just notice them.
“People are always making attempts to get their partners' attention and interest,” Gottman says. In his research, he has found that couples who stay happy (at least during the first seven years) pick up on these cues for attention and give it 86 percent of the time. Pairs who ended up divorced did so 33 percent of the time. “It's the moment we choose to listen to our partner vent about a bad day instead of returning to our television show,” explains Dana R. Baerger, assistant professor of clinical psychiatry and behavioral sciences at the Northwestern University Feinberg School of Medicine. “In any interaction, we have the opportunity to connect with our partner or to turn away. If we consistently turn away, then over time the foundation of the marriage can slowly erode, even in the absence of overt conflict.”
#4 Ignore the bad, praise the good.
Observations of couples at home reveal that people who focus on the negative miss many of the positive things that their partners are doing. Happy spouses, however, ignore the annoyances and focus on the good. “If your wife is irritable one morning, it's not a big deal. It's not going to become a confrontation,” Gottman says. “Then when she does something nice, you notice and comment on that.” Guess what that breeds? More of the good stuff.